Question of the Week: “It’s been more than a year since my last rituximab infusion and my CD20 count is back in the normal range. Why do I not have any signs of an IgG4-RD flare?”
We are pleased to share another edition of the IgG4ward! Question of the Week (QoW) series! This week's QoW and its answer are below. We invite you to join the Online Community and share any follow-up questions or comments you might have about the QoW there.
“It’s been more than a year since my last rituximab infusion and my CD20 count is back in the normal range. Why do I not have any signs of an IgG4-RD flare?”
This excellent question affords us the opportunity to talk a bit about B cell depletion.
B Cell Depletion
B cell depletion is the type of treatment strategy represented by medications such as rituximab and inebilizumab. Before we proceed, it is important to note that neither rituximab nor inebulizumab has been approved at this time by regulatory agencies such as the U.S. Food & Drug Administration (FDA) or the European Medicines Agency (EMA).
Rituximab and inebilizumab are antibodies designed for therapeutic purposes that target specific proteins found only on the B lymphocyte family of cells. B lymphocytes, which are a subset of our bodies’ white blood cells, are critical to the disease mechanisms of IgG4-RD. Rituximab works by binding to a cell-surface protein known as “CD20” (CD is an abbreviation for both “cluster of differentiation” and “classification determinant.”). The binding of rituximab to CD20 to a B cell marks the bound cell for destruction (“depletion”) by other components of the immune system. A schematic of the CD20 protein on the B cell surface is shown in the figure.
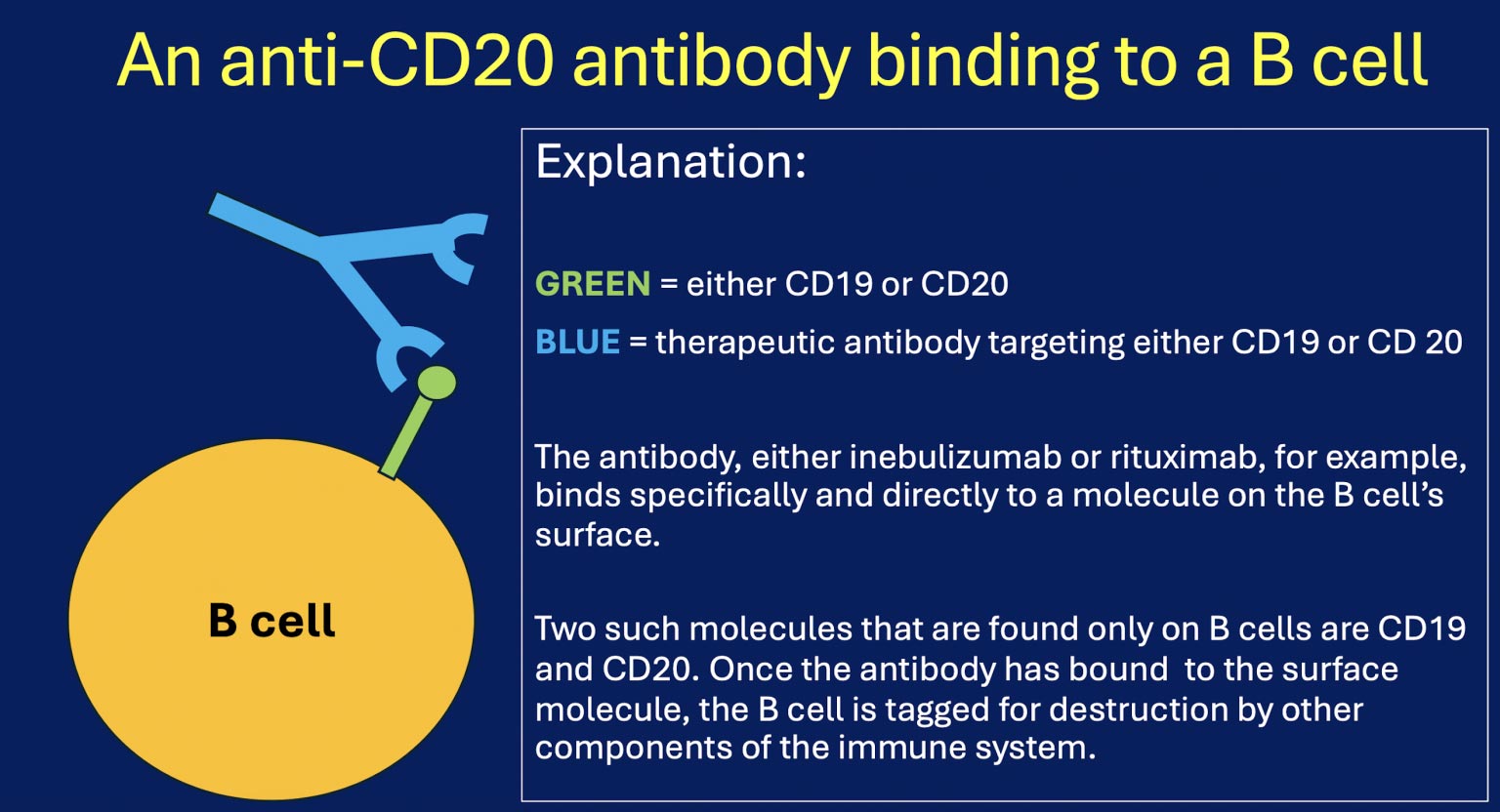
Inebulizumab works in a manner that is similar to that of rituximab. Rather than binding to CD20, however, inebulizumab binds to another target on the B cell surface, namely CD19. Both CD19 and CD20 are proteins that are unique to B cells, so targeting them allows these medications to limit its effects largely to these cells. This reduces much of the “collateral damage” or “off-target effects” that can be associated with treatments that are less specific, such as steroids (prednisone).
A few key points:
Within days of a person’s receiving a B cell depletion treatment, measurable B cells disappear from the blood circulation.
The currently available B cell depletion agents do not eliminate all B cells from the body. Even though B cells are no longer measurable in the blood, B cells persist within tissues such as lymph nodes.
Nevertheless, simply eliminating B cells from the peripheral blood can have dramatic effects on disease activity in a number of conditions, including IgG4-RD. These positive effects on disease activity last for a variable amount of time. The duration can be only a few months in some patients, but up to several years in others. The variables that determine length of response in a given patient remain incompletely understood.
The B Cells Come Back
B cells inevitably return to the peripheral blood eventually, although as noted the time when this “repletion” occurs varies from person to person. Now, here is the point that addresses the Question of the Week directly: the return of B cells to the blood circulation does not always correlate with the return of disease. Some patients can remain asymptomatic for months or years after B cells are once again detectable in the blood. This may be because: 1) the disease-causing B cells were eliminated with great efficiency and thoroughness by the initial treatment; and, 2) it takes a while for a troublesome subset of B cells to reappear.
In a minority of patients, active disease may appear again quickly after B cell recovery (for example, within 3 months). Because of the imperfect relationship between B cell levels in the blood and the overall IgG4-RD activity, blood levels of IgG4 appear to be a more reliable marker than B cell levels of disease activity for most patients, at least with our current measurement techniques.
In summary, regular monitoring of B cell levels in the blood is not particularly helpful most of the time in clinical settings. In contrast, monitoring blood levels of IgG4 at regular intervals is extremely helpful in many people living with IgG4-RD.
Please let us know if these answers are helpful (and, of course, if they raise additional questions! Please post any follow-up questions in the Online Community).