Should IgG4-RD patients worry about infections such as Pneumocystis jiroveci pneumonia (PJP)?
Our Question of the Week this week comes from China. Thank you, Hua, for posing it:
“I have questions regarding the increased risk for opportunistic infections caused by immunosuppressive medications. I read a paper saying that long-term use of steroids for transplantation patients may occasionally cause PjP (Pneumocystis jiroveci pneumonia), a lung infection that can be fatal.
It makes me very anxious to be honest, because for IgG4 RD patients like us, the long-term use of steroids is so common even though the doses are tapered over time and hopefully stopped in the end.
Should IgG4-RD patients worry about infections such as PJP? If so, is it necessary to take preventative medicines such trimethoprim/sulfamethoxazole when taking high-dose glucocorticoids?
What other ways that we could use to reduce risk for opportunistic infections in general?”
Hua, your question is highly relevant for the great majority of IgG4-RD patients around the world, for whom glucocorticoids (steroids) remain the cornerstone of treatment.
One of the most concerning potential side-effects of steroid use is an increased risk of infection, and this ranges from everything to hospitalization for pneumonia to a higher risk of zoster (shingles) and many other types of infectious risks. We have discussed some of the other specific risks associated with low-dose steroid use in a previous question of the week. You can review that information here.
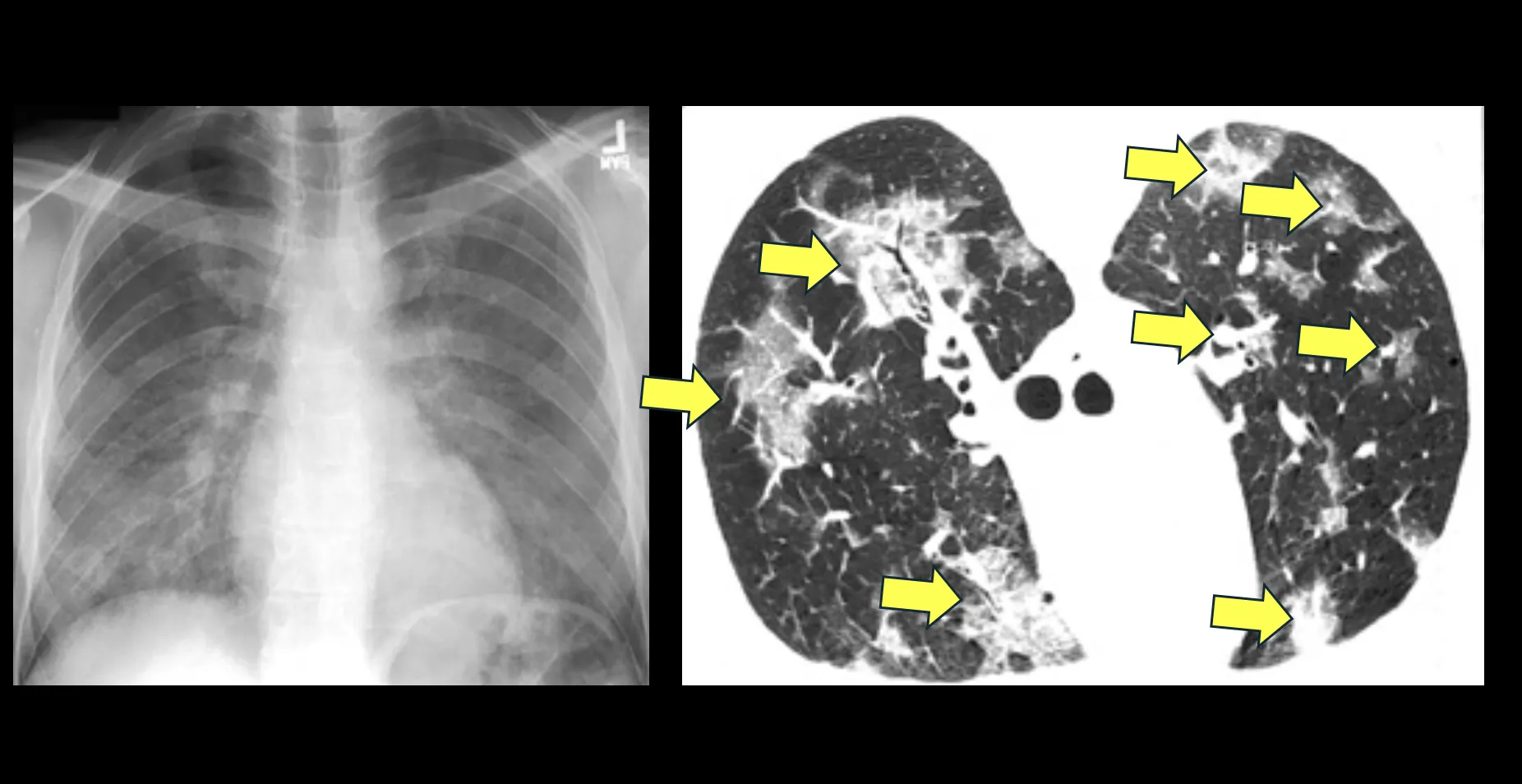
Your question about PjP (Pneumocystis jiroveci pneumonia) makes me think back to the early days of the AIDS epidemic – the mid-1980s through the mid-1990s – when I was a medical intern and infections from this opportunistic organism, then called Pneumocystis carinii or PcP were the leading cause of death among AIDS patients. Many thousands of AIDS patients – probably millions, in fact – died very quickly from overwhelming PcP infections because their immune systems had become severely compromised by the human immunodeficiency virus (HIV). Some chest X-rays and chest CT images from patients with severe Pneumocystis infections are shown in the Figure.
Fortunately, the risk of Pneumocystis jiroveci pneumonia in people living with IgG4-RD is far, far lower. This is primarily because the doses of steroids (prednisone, prednisolone) used to treat IgG4-RD are usually kept at moderately high doses – usually starting at 40 mg/day of prednisone – before tapering begins after about a month. The risk of severe short-term side-effects of steroids is related directly to the prednisone dose and to the duration of treatment at that dose.
Most patients with IgG4-RD in general practice are able to taper to 5-10 mg/day within a couple of months, meaning that their window of vulnerability to severe opportunistic infections such as PJP is pretty narrow and the likelihood of such an infection is low.
We do not usually use prophylactic antibiotics to prevent such infections in IgG4-RD patients because antibiotics themselves can be associated with side-effects and because the optimal prevention strategy in IgG4-RD is simply to taper the prednisone to a low dose.
As we have emphasized in other discussions of steroids, the use of even low doses (e.g., 5 mg/day of prednisone) can be associated with a number of other important adverse effects, but opportunistic infections such as PjP at such doses are rare in the absence of extenuating circumstances.
Hope this is helpful. Please let us know if you need any clarification or have follow-up questions
Stay up to date with the question of the week and the latest happenings within the IgG4-RD community by joining the IgG4ward! Online Community.