Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Organ affected: pancreas
Pancreas and bile duct inflammation that can mimic cancer: symptoms, key tests, and why early treatment matters.
 6 lessons
6 lessons Total: tbc
Total: tbc 10 minutes + videos
10 minutes + videosPancreas overview
Understand the pancreas, autoimmune pancreatitis, and the key steps doctors use to reach a clear diagnosis.
Understanding IgG4-RD in the pancreas and autoimmune pancreatitis
If you’ve been told you may have autoimmune pancreatitis (AIP), it’s completely reasonable to have questions. When IgG4-related disease (IgG4-RD) involves the pancreas, it often shows up as slow, immune-driven swelling and inflammation, sometimes with vague upper belly discomfort or back pain, weight loss, diabetes, or jaundice (yellowing of the eyes or skin.
Because these same findings can overlap with other pancreatic and bile-duct conditions, including – at times – cancer, your clinicians may recommend a careful, stepwise workup. A biopsy is sometimes part of that process to confirm what the tissue shows and to guide the safest next steps.
In this lesson, we’ll discuss:
what the pancreas normally does,
what it looks like when it’s inflamed, and
how IgG4-related disease (IgG4-RD) can involve the pancreas.
We’ll also explain why doctors talk about two types of autoimmune pancreatitis: type 1 is often tied to IgG4-RD, while type 2 usually is not. Imaging, blood tests, and sometimes tissue sampling are often used together to clarify what’s going on.
Fireside Chat: Pancreatic & Biliary Insights in IgG4-related disease
What IgG4-RD in the pancreas can look like
Autoimmune pancreatitis (AIP) is inflammation of the pancreas driven by the immune system. In plain language: the immune system mistakenly treats the pancreas like it’s under attack, causing swelling and irritation.
In IgG4-RD, that swelling can be slow and “quiet” at first. Some people feel vague upper belly discomfort or back pain. Others notice weight loss or new/worsening diabetes. Some people first notice jaundice (yellowing of the eyes or skin) because inflammation in or near the pancreas can squeeze the bile duct like a kinked garden hose.
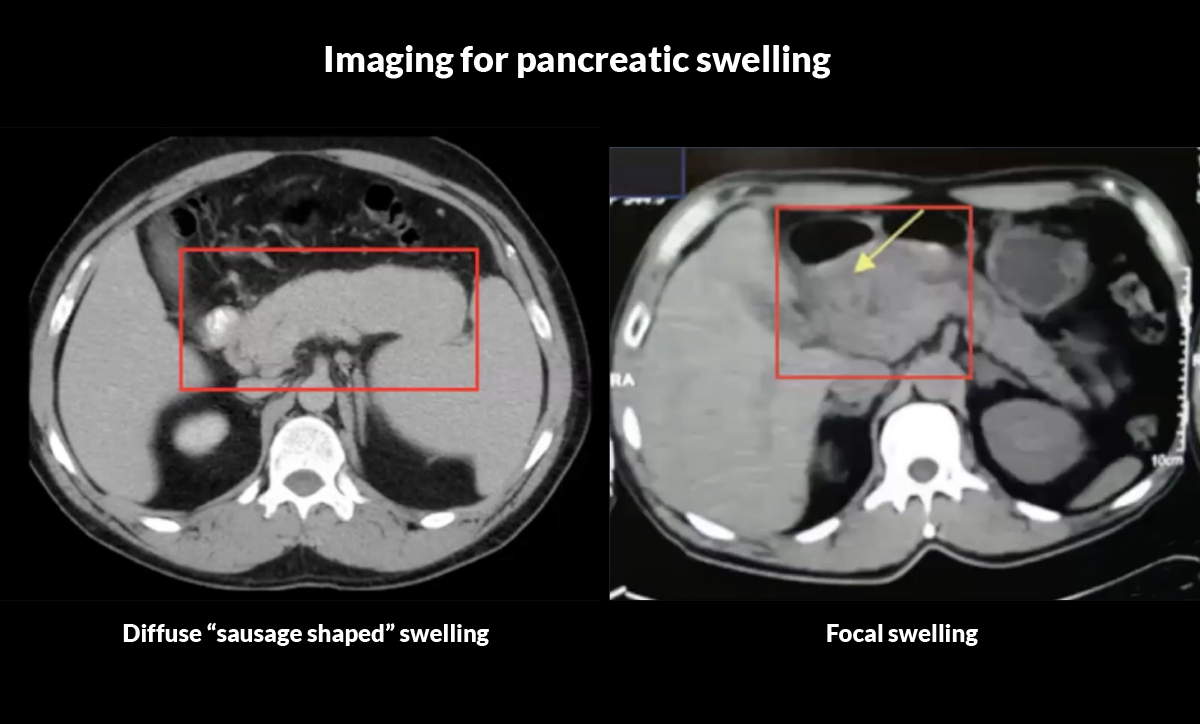
A key reason AIP gets so much attention is that it can sometimes form a mass-like area in the pancreas.1 That can look like pancreatic cancer on scans, which is one reason doctors take it so seriously.
How common is it?
Pancreatic and bile-duct involvement is one of the more common patterns doctors see in IgG4-RD. 1
About 40% of people with IgG4-RD develop autoimmune pancreatitis, and many also have inflammation in the bile ducts (IgG4-related cholangitis). 2
What is the anatomy like?
The relationships between the pancreatic duct and the bile ducts (which emerge from the liver) are shown in the Figure below. The hepatic (liver) bile duct emerges from the liver and merges with the pancreatic duct to form the common bile duct. The common bile duct collects bile and digestive enzymes from both the liver and the pancreas, empytying them into the small intestine to aid the normal digestion of food.
The pancreas is situated right in the center of things, in the center of the abdomen, located in the retroperitoneum (the space behind the abdominal cavity). Doctors think of the pancreas as being divided into a head (the part closest to the common bile duct, toward the right side of the body), a body (the mid-portion), and a tail (the end of the pancreas, over toward the left side of the body). This concept is important because radiologists often describe pancreatic inflammation or masses as being localized to the head of the pancreas, to the tail of the pancreas, etc. Sometimes, the entire pancreas is inflamed.
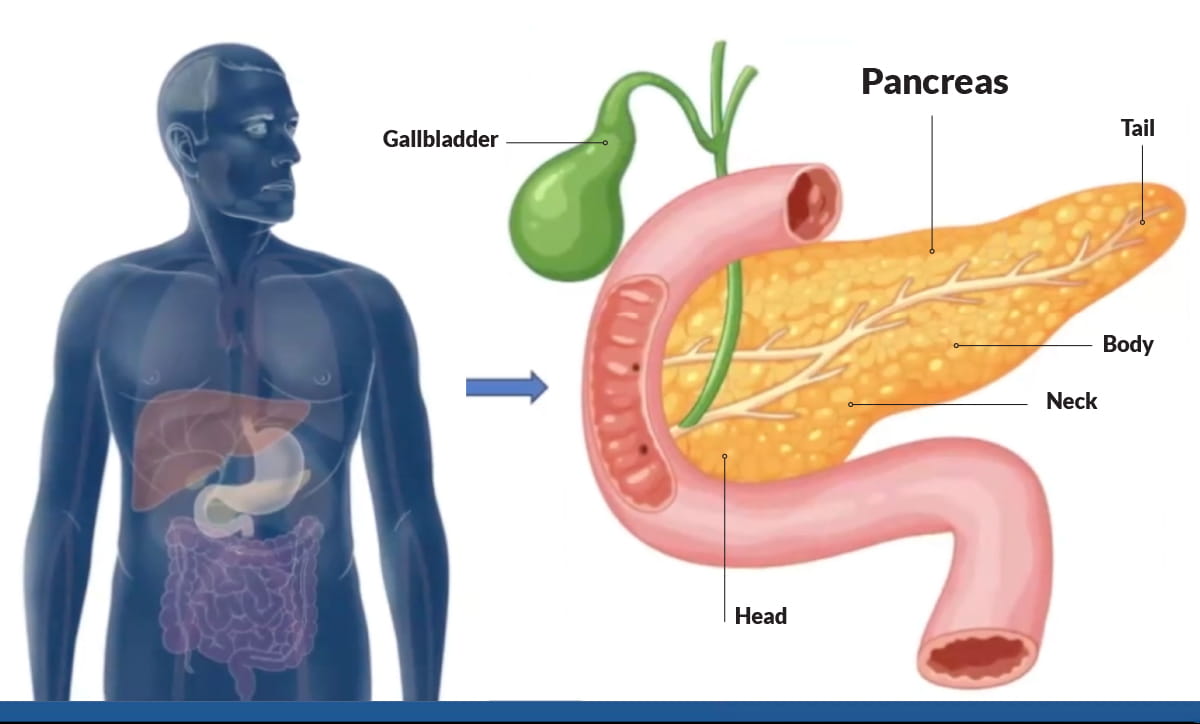
The pancreas helps you digest food and regulate blood sugar.
What the pancreas normally does
The pancreas is an organ that makes digestive enzymes and blood-sugar hormones (including insulin). What that means in plain language is that the pancreas helps your body digest food and absorb nutrients, and also regulates your blood sugar (glucose) concentration. Both of these are vital processes.
The pancreas has two main functions:
1) Digestion (the exocrine function)
It makes enzymes that travel through the pancreatic duct into the common bile duct, and from there into the first part of the small intestine (the duodenum). Pancreatic enzymes are essential for the digestion of food, especially fats, which are hard to digest properly without the pancreas.
2) Blood sugar control (the endocrine function)
It makes hormones, especially insulin, that go directly into the bloodstream to help regulate blood sugar. Cells in the pancreas sense the concentration of glucose in the blood and time the release of insulin immaculately to help maintain normal glucose control. Disruption of this process leads to “glucose intolerance,” or diabetes mellitus (diabetes).
Bile duct involvement: Because the head of the pancreas sits right next to the common bile duct, inflammation in the pancreas can squeeze the duct, causing a blockage of bile flow into the small intestine. A blockage of bile flow leads to jaundice, a yellowing of the eyes and skin.
IgG4-RD linked to inflammation in the pancreas
When IgG4-RD affects the pancreas, it often shows up as a specific form of AIP called type 1 autoimmune pancreatitis.
That connection matters because it changes what your care team looks for. If your AIP is type 1, your clinicians may also check for signs of IgG4-RD in other places, especially the bile ducts, because the pancreas and bile ducts are often involved together (sometimes called a pancreaticobiliary pattern).
The identification of type 1 IgG4-related AIP means that the doctor should investigate the possibility that IgG4-RD is present in other organs: the organs of the head and neck (major salivary glands, lacrimal glands, orbits, etc.), organs of the chest (lungs, aorta), and other abdominal organs. This may involve additional blood tests, imaging studies of other organs, consultation with a rheumatologist, and other evaluations.
Autoimmune pancreatitis is the medical term to describe inflammation of the pancreas that is immune-mediated, meaning the immune system is driving the inflammation.
Experts describe type 1 AIP (the IgG4-related form) as “antigen-driven,” meaning that something – an antigen – has triggered the immune system to become active against a portion of the patient’s own body. In IgG4-RD, the exact trigger(s) isn’t clearly known.
Over time, inflammation can shift into a more fibrotic phase, which is scarring that can cause more lasting damage if the disease isn’t controlled.
Two types of autoimmune pancreatitis
One of the most important things to know is that AIP is not one single disease. There are two main types, and they don’t refer to the same disease.
Type 1 AIP: the IgG4-related form
Type 1 AIP is the form that is most strongly linked to IgG4-RD. It is also the more common type. It can be associated with inflammation in other organs, particularly the bile ducts (for example, sclerosing cholangitis), and sometimes the salivary glands or kidneys. If your doctor says “this looks like IgG4-related pancreatitis,” they are talking about type 1 AIP.
Type 2 AIP: usually not IgG4-RD
Type 2 AIP is less common than type 1 and is usually focused exclusively on the pancreas rather than tending to involve other organs, too, as IgG4-RD often does. This is why the distinction between type 1 and type 2 AIP matters. Type 2 AIP is a form of autoimmune pancreatitis, but it does not carry the same possibility of other organ involvement, as is true for type 1.
Feature | Type 1 AIP (LPSP) | Type 2 AIP (IDCP) |
|---|---|---|
How common is it? | 85–90% of AIP cases | 10–15% of AIP cases |
Full name | Lymphoplasmacytic sclerosing pancreatitis (LPSP) | Idiopathic duct-centric pancreatitis (IDCP) |
Is it part of a whole-body illness? | Yes. Often part of IgG4-related disease (IgG4-RD) (can involve multiple organs) | Usually no. More pancreas-focused |
What doctors see under the microscope (hallmark) | Often shows storiform fibrosis (a “whorled” scarring pattern), obliterative phlebitis (inflamed/blocked veins), and increased IgG4+ plasma cells | Often shows a granulocytic epithelial lesion (GEL), which is considered very characteristic (pathognomonic) for type 2 |
Typical age/sex pattern | Often over 60, more common in men (about 2:1) | Often 40–50, men and women about equal |
Serum IgG4 blood level | Often elevated (about ~80% of cases) | Usually normal |
Other organ “clues” | May be associated with IgG4-related sclerosing cholangitis (bile duct inflammation/scarring), sialadenitis (salivary gland inflammation), nephritis (kidney inflammation), retroperitoneal fibrosis, and any of the other organ manifestations of IgG4-RD. | May be associated with inflammatory bowel disease (IBD) in ~30% of cases |
Relapse (flare coming back after treatment) | Higher relapse risk, likely well over 50%. | Very low relapse risk (<10%) |
Symptoms seen with pancreatic inflammation
When the pancreas is inflamed or scarred, symptoms often line up with the pancreas’s two jobs:
If enzyme function drops (exocrine insufficiency): People may get bloating, cramps, diarrhea, and later fatty stools that can look greasy or pale/clay-colored. They may lose substantial amounts of weight and become malnourished.
If insulin function drops (endocrine dysfunction): Blood sugar can rise, and diabetes can appear or worsen.
Ironically, the exocrine and endocrine function can have a “Yin/Yang” relationship. As the effects of exocrine pancreatic failure worsen and patients lose more weight, becoming malnourished, the endocrine function is less stressed and blood sugar control may become less impaired. This is not the optimal way, however, to manage the diabetes that sometimes results from IgG4-RD!
Symptom or change | What it may look like in real life |
|---|---|
Changing pain pattern | Pain that is new, more frequent, more severe, or feels different than before |
Weight loss unresponsive to enzyme replacements | Ongoing weight loss even after taking pancreatic enzyme pills as prescribed |
Development of biliary and/or gastric outlet obstruction | New jaundice/itching/dark urine (bile duct blockage) and/or vomiting/early fullness (stomach outlet blockage) |
New onset of diabetes | New diagnosis of diabetes or a sudden worsening of blood sugar control |
Why AIP can be hard to diagnose
From the medical side, the challenge is that AIP can mimic other conditions, especially pancreatic cancer, with presenting symptoms and on imaging.
Diagnosis usually requires putting several clues together, such as:
your symptoms and physical examination (there may be readily-apparent clues to the diagnosis of IgG4-RD in other organs, e.g., the submandibular glands)
imaging (CT/MRI, sometimes PET)
blood tests (including IgG4 levels)
sometimes a biopsy, often guided by endoscopic ultrasound
If the road to diagnosis has felt long—or stressful—you’re not alone. AIP is one of the classic “great mimics” in IgG4-RD, and careful evaluation is important to rule out more aggressive conditions. 1,3
When AIP mimics pancreatic cancer
AIP can form a pancreatic mass and cause painless jaundice, which is also a classic presentation of pancreatic cancer in older adults. This means many IgG4-RD patients are initially told they might have cancer – terrifying words that no one wants to hear. That’s why further testing is critical.
Blood tests can help, but they aren’t conclusive. IgG4 levels may be normal, including in situations where a tumor-like mass has formed, so clinicians often can’t rely on a single lab result.
So doctors combine multiple diagnostic tools and observations: imaging, blood work, symptoms, other organ involvement, and—when needed—biopsy, often using endoscopic ultrasound to sample tissue.
Inflammation can look like a mass on imaging, which is why biopsy may be needed.
Other clinical symptoms support IgG4-RD diagnosis
When doctors suspect type 1 autoimmune pancreatitis (AIP), they don’t just look at the pancreas. They also look for “clues” outside the pancreas, because IgG4-RD can involve several organs.
Common extra-pancreatic findings include:
bile duct inflammation/scarring (sclerosing cholangitis)
salivary gland enlargement
enlarged lymph nodes (lymphadenopathy)
kidney inflammation (tubulointerstitial nephritis)
retroperitoneal fibrosis (scar-like inflammation in the tissue behind the abdomen)
lung nodules or masses
The reason this matters is practical. If someone has pancreatic inflammation and a pattern like bile duct involvement (for example, sclerosing cholangitis) or salivary gland swelling, that combination can strengthen the case for IgG4-RD–related AIP and help clinicians choose the right next tests.
It’s also a reminder that symptoms may come from more than one place, so if you’ve noticed issues such as swelling of the area around the eyes, gland enlargement, or evidence of a slow-down in kidney function, they aren’t “random.” They may be part of one connected immune pattern that your care team can evaluate and treat.
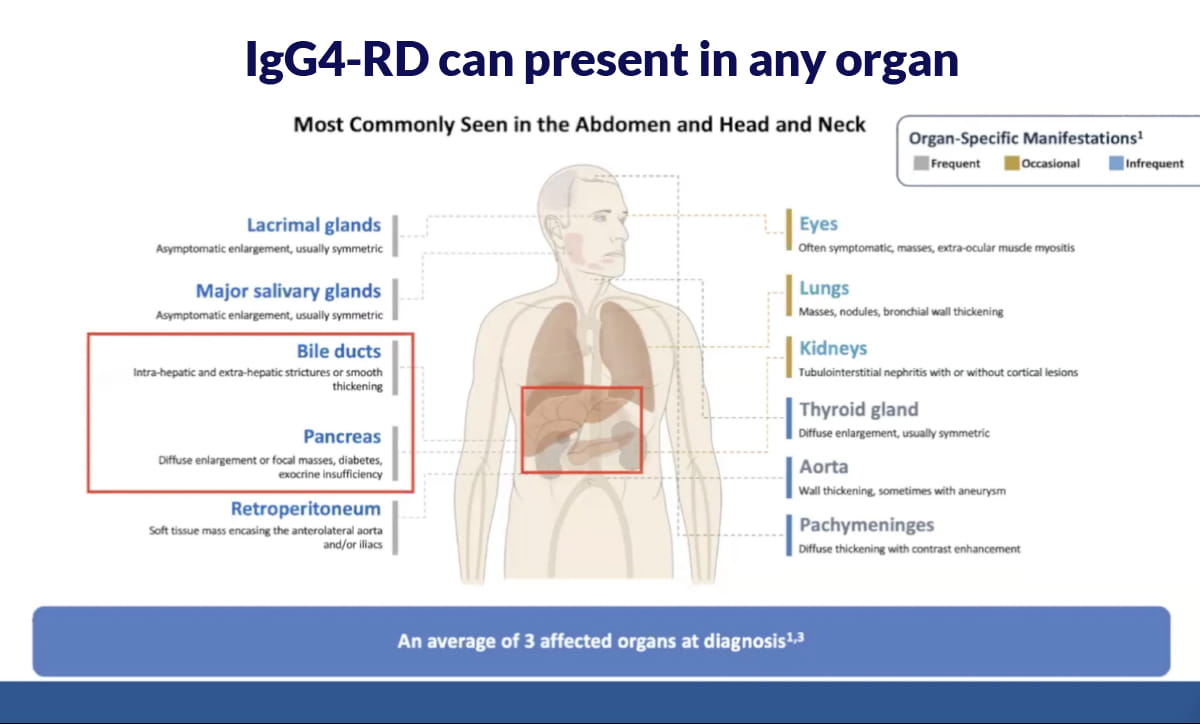
With type 1 autoimmune pancreatitis (AIP), other organs are often affected.
Summary
The pancreas helps with digestion and blood sugar control, and IgG4-RD can inflame it in a way called type 1 autoimmune pancreatitis. Because AIP can form a mass and mimic cancer on imaging, doctors often need to combine scans, labs, and sometimes biopsy to reach the right diagnosis.
In the next lesson, we’ll hear from patients who have experienced these issues.
References
1. Stone JH, Zen Y, Deshpande V. IgG4-Related Disease. New England Journal of Medicine. 2012;366:539–551. doi:10.1056/NEJMra1104650. https://doi.org/10.1056/NEJMra1104650
2. Katz G, Harvey L, Hernandez-Barco YG, et al. Defining pancreatic damage and symptom burden in IgG4-related autoimmune pancreatitis: A cross-sectional study of 118 patients from a single-center registry. Seminars in Arthritis and Rheumatism. 2025;73:152742. doi:10.1016/j.semarthrit.2025.152742. https://doi.org/10.1016/j.semarthrit.2025.152742
3. Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. The Lancet. 2015;385(9976):1460–1471. doi:10.1016/S0140-6736(14)60720-0. https://doi.org/10.1016/S0140-6736(14)60720-0
4. He X, Zhang J, Liu Y, et al. Clinical characteristics and organ involvement patterns in IgG4-related disease with autoimmune pancreatitis. Pancreatology. 2022;22(2):202–209. https://www.sciencedirect.com/science/article/abs/pii/S1424390321006530?via%3Dihub
Get the IgG4ME! app
Keep your IgG4-RD story organized in one place. Track your history, labs, and care team so you can share what matters when it matters most.
Download app now