Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Organ affected: salivary & lacrimal glands
How IgG4-RD swells tear/ saliva glands, how it differs from Sjögren’s or infection, and what helps most.
 6 lessons
6 lessons Total: tbc
Total: tbc 10 minutes + video
10 minutes + videoOrgan overview
Learn what these glands do, why they swell in IgG4-RD, symptoms to watch for, and how doctors confirm the diagnosis.
Salivary and lacrimal gland involvement in IgG4-RD
When your face looks puffy near the jaw, or your eyelids look swollen, it can be scary. Many people immediately think, “Is this an infection? A tumor? Cancer?” That reaction makes sense, IgG4-RD can look like other problems at first.
One reassuring pattern doctors often see is that IgG4-RD in these glands tends to build slowly over months rather than appearing overnight. And once it’s recognized, there are effective ways to calm inflammation and protect function.
In this lesson, we cover:
what the salivary and lacrimal glands do normally
how IgG4-RD can affect them (swelling, dryness, “mass-like” changes)
what this can mean for you day to day and over time
how doctors sort IgG4-RD from look-alike conditions
How common is it?
Across large studies of people with IgG4-RD, head and neck involvement shows up often. Swelling of the salivary glands and tear glands is one of the most common patterns doctors see.
Salivary and lacrimal gland involvement is not a “rare corner” of IgG4-RD. It’s a common part of the story for many people. Among patients in a large clinical trial group and a large international research group used to build classification criteria, studies1 found:
About 50% of patients had submandibular (salivary) gland involvement
About 40% of patients had lacrimal (tear) gland involvement
About 53% of patients had head and neck involvement overall
Understanding a few medical terms
Before we dive in, let’s define a few medical terms so the rest feels easier to follow.
Sialadenitis (inflammation of a salivary gland)
The saliva-making glands get inflamed and may swell. People often describe a slow-growing fullness, not a sudden “infection-like” flare. In IgG4-RD, this may involve:
submandibular glands (under the jaw)
parotid glands (near the ear)
sublingual glands (under the tongue)
Dacryoadenitis (inflammation of the lacrimal gland)
The tear-making gland gets inflamed. In IgG4- RD, this can show up as swelling near the outer upper eyelid, sometimes with a heavy or puffy feeling around the eyes.
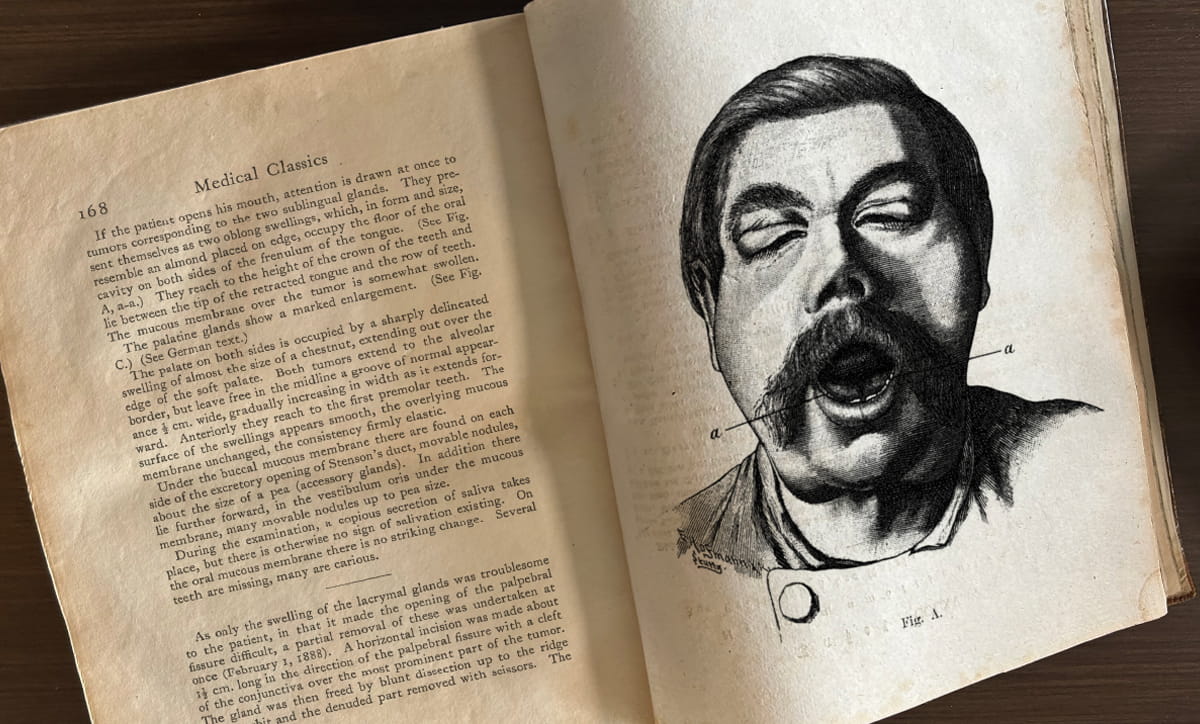
Mikulicz disease (older term)
A historical name used before IgG4-RD was recognized as one condition. It refers to the pattern of both salivary and lacrimal gland enlargement. The first patient in the medical literature recognized—in retrospect—to have IgG4-RD actually had involvement of all three glands: lacrimal, parotid, and submandibular. The patient was a 44-year-old German farmer whose case was described in 1892 by Dr. Joseph Mikulicz. It was only in the first few years of THIS century that “Mikulicz disease” was actually known to be caused by IgG4-RD affecting these glands.
Sjögren's syndrome (autoimmune condition that targets glands)
The immune system mainly attacks the tear and salivary glands, so dry eyes and dry mouth are usually the dominant symptoms. It can look similar to IgG4-RD gland disease, which is why doctors sometimes consider both when evaluating swelling or dryness.
For many decades, Mikulicz disease was considered to be a variant of Sjögren's syndrome. In fact, these two diseases are completely separate conditions, with very different treatments. So it is important to differentiate them and diagnose them correctly.
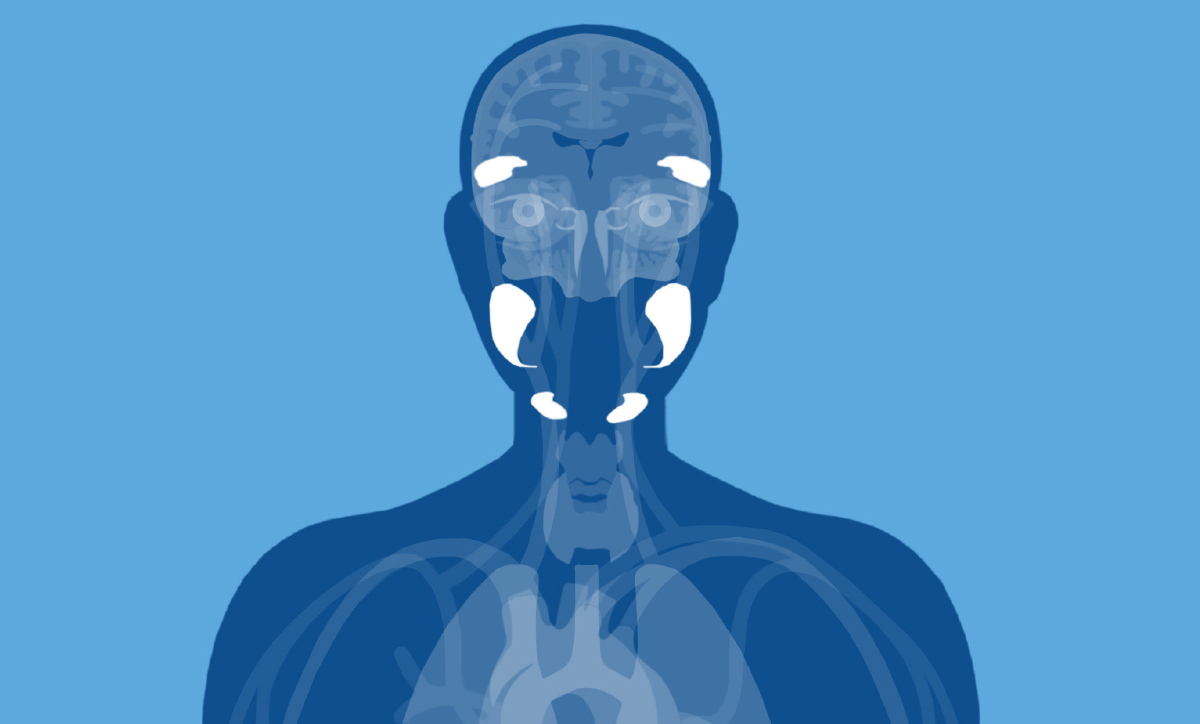
What these glands do normally
Salivary glands make saliva. Saliva helps you chew and swallow, protects your teeth, and keeps your mouth comfortable. The major salivary glands include the parotid glands (in front of the ears) and the submandibular glands (under the jaw). There are also sublingual glands (under the tongue) that can be overlooked, but they matter too.
Lacrimal glands make tears. Tears protect the surface of the eye and help keep vision clear and comfortable. Sometimes IgG4-RD affects more than just the tear gland. It can also involve the nearby soft tissues in the eye socket (the orbit), including the muscles that move the eye and tissue around small nerves, which can lead to eye bulging, double vision, or eye pain.
How IgG4-RD affects salivary and lacrimal glands
Inflammation is the medical term for an immune “alarm response.” In IgG4-RD, that alarm can misfire and keep blaring in certain tissues. Over time, inflammation can lead to fibrosis, which is scar-like tissue that can make an organ stiffer.
In the salivary and lacrimal glands, IgG4-RD often shows up as gradual swelling. It is commonly on both sides, though not always. In lacrimal disease, eyelid swelling (edema) can be very noticeable.
You may also hear older terms:
Dacryoadenitis: another term for lacrimal gland enlargement/inflammation
Mikulicz disease: an older term used when both lacrimal and major salivary glands are enlarged
What symptoms might feel like in real life
People often describe :
swelling under the jaw or near the ears (salivary glands)
puffiness of the upper eyelids or fullness near the outer corner of the eye (lacrimal glands)
dry mouth or dry eyes, which can range from mild to bothersome
Differentiating from Sjögren's syndrome
A practical clinical note: gland swelling in IgG4-RD is sometimes confused with Sjögren's syndrome, another condition that affects these glands. Dryness in IgG4-RD is often described as milder and sometimes improving with treatment, while Sjögren dryness is typically more severe and persistent
A doctor explains
As Dr. Matthew C. Baker explains in this video, dryness in IgG4-RD can happen, but it is often milder and may improve with treatment, while dryness in Sjögren syndrome is typically more severe and tends to persist.
Orbital and soft tissue around the eyes
Sometimes IgG4-RD doesn’t stop at the tear gland. It can also involve the orbit, which is the “socket” area that holds the eye and the soft tissues that help the eye move and function. When inflammation shows up here, it can affect the eye-movement muscles, other orbital soft tissue, and even tissue around nerves.
This can cause a bulging eye (proptosis), double vision, or other vision changes, and sometimes pain or redness if inflammation involves the eye surface (scleritis) or inside the eye (uveitis).
Symptoms (what you might notice):
A bulging or “pushed forward” eye (proptosis)
Vision changes (blurrier vision, trouble focusing)
Double vision (especially when looking in certain directions)
Pain around the eye or with eye movement
Redness of the eye (more concerning if it’s deep, painful redness)

What gland involvement can mean for long-term health
For many people, the biggest impact is comfort and daily function: how your eyes feel, how your mouth feels, and how noticeable the swelling is. The longer-term concern is whether ongoing inflammation could leave behind fibrosis that is harder to reverse. That’s why clinicians watch for changes over time, not just a one-time snapshot.
Another important implication is pattern recognition: IgG4-RD can involve more than one organ system. So even if the glands are what you notice first, your team may look for other organ involvement based on your symptoms and exam.
Expert case: when sinus and tear-duct disease threatens vision
In this video, Dr. John H. Stone speaks with Dr. Bart K. Chwalisz about a 59-year-old man with long-standing sinus disease who developed a blocked tear-duct (tears overflowing) and then sub-acute vision loss with eye pain. MRI showed inflammation affecting multiple nearby areas, and an endoscopic biopsy through the nose confirmed IgG4- RD. With steroids followed by B-cell depletion (rituximab), he improved and avoided permanent vision loss.
Why it can be hard to diagnose
From the patient side, gland symptoms can feel straightforward: “My glands are swollen,” or “My eyes and mouth feel dry.”
From the medical side, the challenge is that gland swelling can look like many other conditions. Some are common and benign. Others are more urgent, like infection or cancer. That’s why clinicians often need to combine your story, the physical examination, imaging studies, blood tests, and sometimes biopsy findings to feel confident in the diagnosis.
IgG4-RD can be a tricky puzzle because it can look different from one person to the next, and its symptoms can overlap with other conditions.
If the road to diagnosis has felt long or uncertain, you’ve come to the right place. This chapter is here to help you make sense of what’s happening. It will give you a better understanding of what patterns to look for, what questions to ask, and what the next steps usually are.
How doctors confirm what’s going on
There isn’t one single test that proves IgG4-RD. Doctors usually need the full picture: what you feel, what they find on exam, what imaging shows, what blood tests suggest, and—most often—what a biopsy shows under the microscope.
Laboratory tests (supportive, not definitive)
Blood work can support the diagnosis and sometimes helps track disease activity, but it can’t confirm IgG4-RD on its own. Common “IgG4-RD labs” include:
IgG subclasses (including IgG4)
IgE
Complement levels (C3 and C4)
It’s interesting to note that serum IgG4 is elevated in about 80–90% of patients at some point, depending on the cohort, and can be a helpful marker when interpreted in context.1 But elevated IgG4 (or lack of) isn’t conclusive on its own.
In many patients, these markers may improve with treatment and shift again when disease returns, but doctors still look for organ-based evidence of active disease, not lab changes alone.
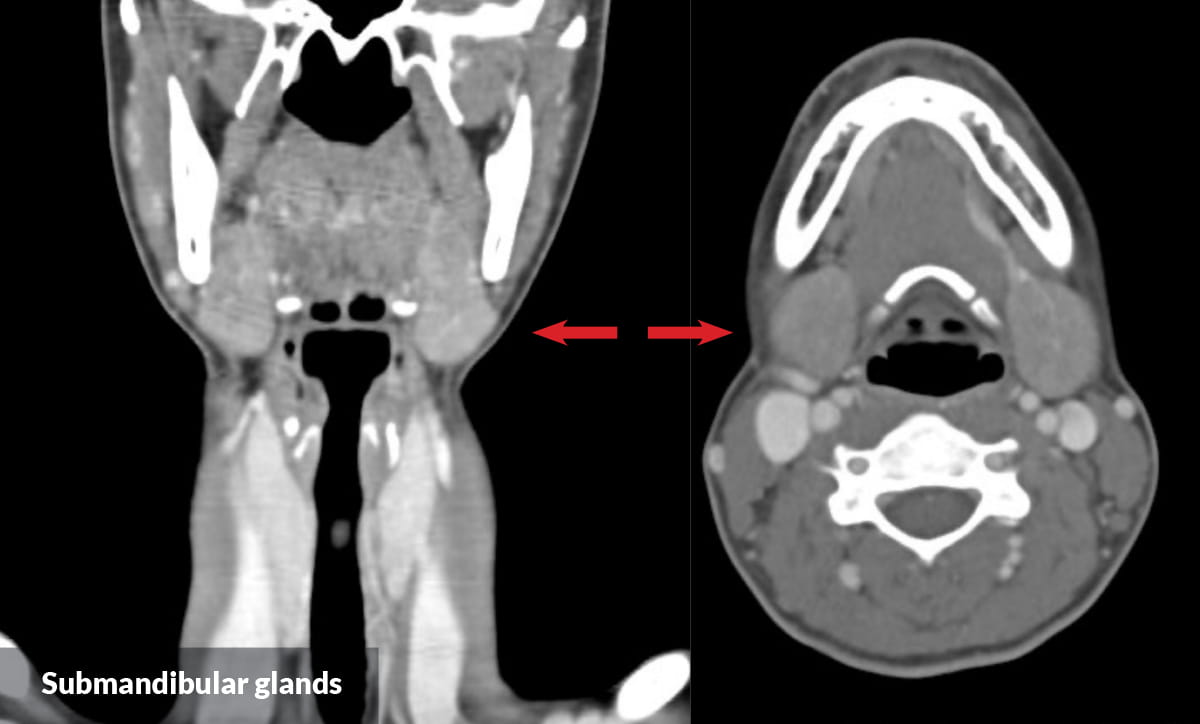
Imaging studies (head and neck focused)
Imaging helps doctors see where inflammation is and how extensive it may be.
CT scan of the neck (often with contrast) can help assess salivary gland and neck involvement.
MRI of the orbits is commonly used when lacrimal glands or orbital tissues may be involved.
FDG-PET/CT may be used in selected situations to look for disease activity in multiple areas of the body.
Pathology (often the key step)
For most patients, a biopsy is the most conclusive way to sort IgG4-RD from look-alike conditions. 1
It’s important to remember that when it comes to diagnosing IgG4-RD: mimics exist. Doctors have to be certain to rule out cancer, so they use several tests to build truly conclusive evidence, not just one lab value or one scan.
That’s why biopsy can be so important: it helps prevent the wrong diagnosis and the wrong treatment.
A few considerations:
If a biopsy was done previously, the original tissue can sometimes be re-reviewed and an IgG4 stain added, so you may not always need a repeat procedure if the specimen can be obtained and re-read by an experienced pathologist.
More tissue is usually better. In general, an excisional biopsy provides the most information, followed by a core biopsy, and then fine needle aspiration (FNA). FNA can be limiting because it often doesn’t provide enough architecture to confirm the pattern.
Lymph node biopsies are often not particularly helpful for the classic IgG4-RD pathology features, even when lymph nodes are enlarged. 1
Lesson 3 discusses treatment options and how the condition is managed.
Summary
Your salivary glands help protect and moisten your mouth, and your lacrimal glands protect and moisten your eyes. In IgG4-RD, these glands can slowly swell and may cause dryness.
Doctors usually diagnose IgG4-RD by putting together your story, physical examination findings, imaging studies, and often biopsy, because other conditions can mimic IgG4-RD.
Treatments aim to calm inflammation early and protect function, with steroids sometimes used short-term and B-cell–targeted therapy often used to reduce relapse and steroid exposure.
References
1. IgG4ward! Foundation. IgG4ward! PeachJAM Video Series – “How Do I Know If My Disease Is Active?” with Dr. Matthew Baker. YouTube. https://www.youtube.com/watch?v=M6ajwc8dFC8
2. Stone JH, Zen Y, Deshpande V. IgG4-Related Disease.N Engl J Med.2012;366:539–551.https://www.nejm.org/doi/full/10.1056/NEJMra11046503.