Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Getting the right diagnosis
Discover how doctors identify IgG4-RD using blood tests, imaging, biopsies, and clinical patterns.
 7 lessons
7 lessons Total: TBC
Total: TBC 8 minutes + videos
8 minutes + videosDiagnosis overview
Learn why IgG4-RD is often missed at first, and how doctors piece together the clues.
The long road to an IgG4-RD diagnosis
Arriving at an IgG4 diagnosis can be a long road. Patients describe it as a winding, foggy journey with detours and false starts. The reason is simple: there is no single yes-or-no test for IgG4-related disease (IgG4- RD). Instead, doctors combine clues, including those from your story and physical examination, blood work, imaging, and sometimes a small tissue sample (biopsy). They then apply careful clinical judgment in correlating information from all of those sources to reach a diagnosis. Sometimes, a series of tests over time an d multiple specialist visits are required, as well.
The diagnostic dilemma in IgG4-RD
In this video Dr. Arezou Khosroshahi, Professor of Medicine and rheumatologist at Emory University, discusses the complexities of diagnosing IgG4-RD. She explains why diagnosis is often such an arduous journey.
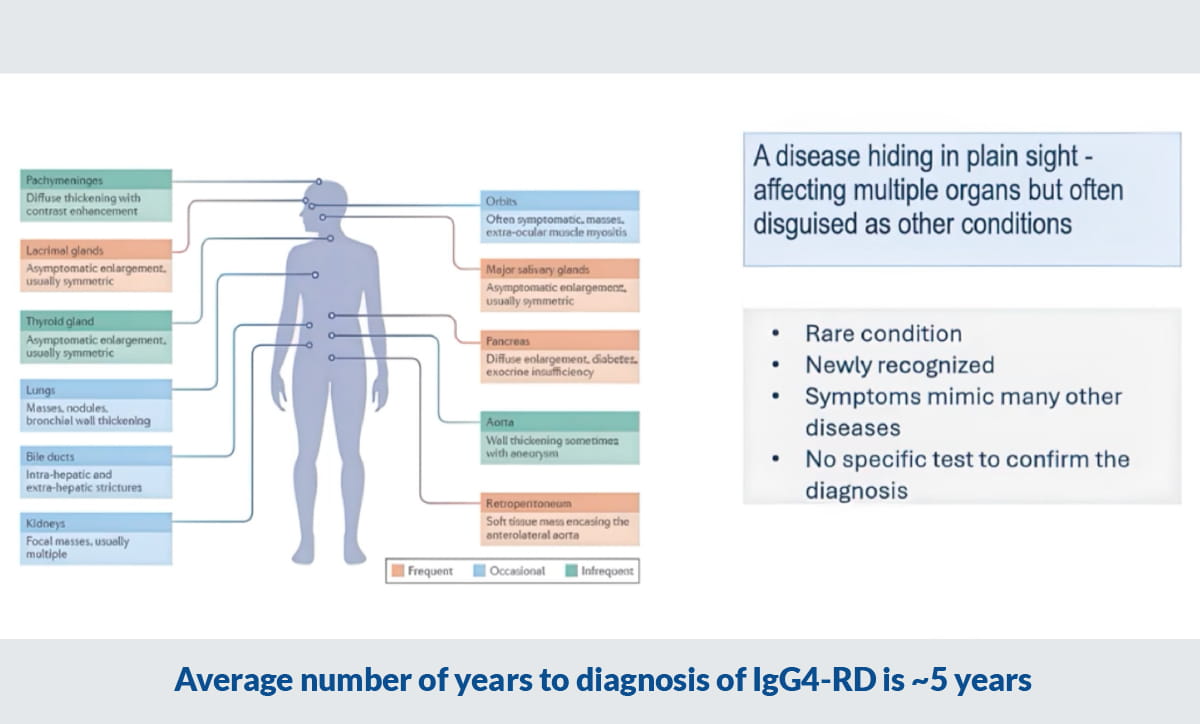
Average number of years to diagnosis of IgG4-RD is ~5 years
Why it’s so hard to diagnose IgG4-RD
Getting to the diagnosis of IgG4-related disease (IgG4-RD) can feel like trying to solve a puzzle when you only have a few pieces at a time. That is not because anyone is “missing” something on purpose, it is because this disease is good at mimicking other conditions, many of which are more common.1,3
In addition, because it’s a systemic disease, IgG4-RD can affect many different organs, leading to a variety of presentations in every person it affects. As you saw in Chapter 1, it took scientists a long time to make the connection between the myriad symptoms and the underlying mechanisms at work in IgG4-RD.
Here are some of the reasons IgG4-Rd is so difficult to diagnose:
1. It’s a multi-organ disease.
IgG4-RD is a multi-organ disease, meaning it can involve many different parts of the body, sometimes all at once, and sometimes one organ at a time over months or years.2,3 It has been described in almost every organ system, including areas such as the pancreas, bile ducts, salivary glands, tissues around the eyes, kidneys, lungs, lymph nodes, the covering around the brain (pachymeninges), and even blood vessels like the aorta.2,4
Because of that, people often land in different clinics depending on their first symptom: GI for jaundice or a pancreas problem, ENT for swollen glands, pulmonology for a lung nodule, nephrology for kidney injury, and so on. No single clinician may see the whole pattern right away.4
2. It hides in plain sight
Second, IgG4-RD often “hides in plain sight” by mimicking other diseases, especially conditions that doctors must rule out quickly, like cancer, serious infections, or other immune diseases (for example, Sjögren’s syndrome or granulomatosis with polyangiitis).1,4,5
A key reason is that IgG4-RD commonly forms mass-like areas of inflammation (doctors may call these tumefactive lesions), and mass-like findings on scans can look frighteningly similar to cancer.2,4 Clinicians usually have to exclude those dangerous look-alikes first, because the consequences of missing cancer or infection are very serious.5
3. There is no definitive test
Third, there is no single “yes/no” test that proves IgG4-RD. Blood tests can help, imaging can help, and biopsies can help, but none of these alone is perfect.1,5 Experts emphasize that diagnosis usually requires putting clues together across:
your story and symptoms
bloodwork (including, sometimes, serum IgG4)
imaging (CT, MRI, PET in some cases)
(often) tissue biopsy, interpreted carefully by experienced pathologists1,5,6
Even the interpretation of biopsies can be tricky in IgG4-RD. The pathological changes of IgG4-RD are sometimes patchy, and some biopsy procedures simply miss the key features (“sampling error”). Correlation between the biopsy findings and the clinical picture is essential.6
4. It’s a rare condition only newly recognized.
Finally, IgG4-RD is still relatively newly recognized as a distinct disease. Many clinicians, therefore—especially those outside of specialty centers—may never have recognized a case before.2,4 In Dr. Stone’s words, if a clinician has never heard of a disease, they are unlikely to think of it when symptoms first appear.4
PATIENT STORY
IgG4‑RD diagnosis changed the course of kidney disease
Christopher Prah first noticed trouble urinating, experienced weight loss, and overwhelming fatigue—symptoms that led to a frightening search for answers as his kidney function worsened. After finally being diagnosed with IgG4-related disease, prompt treatment helped him regain his energy, protect his kidneys, and return to living a full, normal life.
Watch this patient video for deeper understanding.
Steroid response can offer clues
One of the most helpful “real‑world” clues that a person may have IgG4‑RD, is rapid response to glucocorticoids (steroids). Because IgG4‑RD inflammation often improves quickly when treated with steroids, doctors may use a short, carefully monitored course to see if the pattern fits.
If a person doesn’t improve as expected, that’s a signal to pause and re‑check for important mimics, including infection or cancer, or to look for damage (scar tissue) that won’t reverse even when inflammation is controlled.
At the same time, steroid response is not specific—many conditions can look better on prednisone—so clinicians treat it as one piece of evidence, not the final word.
Personalized support on your steroid journey
Get support and education on your steroid journey with a new digital companion, Sam (Steroids and Me). Find answers and learn how to work with your doctors for the best care and taper plan.
Get Sam nowThe tests used for diagnosis
After considering your history and physical examination, physicians may do a series of tests that may include:
Blood tests
Biomarkers in your blood are signposts: IgG4 may be high—or normal—while complement proteins C3 and C4 may run low when the immune system is highly active (especially if multiple organs are affected). The IgE concentration—a level of another antibody—is also sometimes very elevated in IgG4 ‑ RD, though it usually trends in the same direction as IgG4. Eosinophils and ESR add context but aren’t specific to IgG4-RD.
CT/MRI/PET scans
Imaging can reveal organ swelling, masses, or inflammation, and help doctors choose the safest, most informative spot for a biopsy. Images alone can’t diagnose the disease, but they can offer a compelling clue to map the disease footprint (its extent).
Biopsy
Taking a small tissue sample may show classic patterns: dense immune cells, storiform (woven) fibrosis, and inflamed vein walls that help doctors diagnose with confidence. Sometimes getting a good tissue biopsy isn’t possible because the affected tissue is not accessible, and other times even a good attempt at a biopsy does not yield informative tissue. In such cases, doctors have to rely on the clues from other areas.
Another part of the diagnostic puzzle are classification criteria. Continue to the next lesson to learn more.
Get the IgG4ME! app
Keep your IgG4 RD story organized in one place. Track your history, labs, and care team so you can share what matters when it matters most.
IgG4ME appReferences
1. Lang D, Zwerina J, Pieringer H. IgG4‑related disease: current challenges and future prospects. Ther Clin Risk Manag. 2016;12:189–199. doi:10.2147/TCRM.S99985. URL: https://doi.org/10.2147/TCRM.S99985
2. Stone JH, Zen Y, Deshpande V. IgG4‑Related Disease. N Engl J Med. 2012;366:539–551. URL: https://doi.org/10.1056/NEJMra1104650
3. Abo-Helo N, Toubi E. IgG4-related disease: case report and literature review. Autoimmune Highlights. 2015;6:7–15. doi:10.1007/s13317-015-0069-3. URL: https://doi.org/10.1007/s13317-015-0069-3
4. IgG4ward! Foundation. IgG4-RD and Treatment | Fireside Chat Recap + Downloadable Guide. Original air date June 6, 2025. URL: https://igg4ward.org/resources/igg4-rd-and-treatment-fireside-chat-recap-plus-downloadable-guide/
5. Peyronel F, Della‑Torre E, Maritati F, et al. IgG4‑related disease and other fibro‑inflammatory conditions. Nat Rev Rheumatol. 2025;21:275–290. doi:10.1038/s41584-025-01240-x. URL: https://doi.org/10.1038/s41584-025-01240-x
6. Arias-Intriago M, Gomolin T, Jaramillo F, et al. IgG4-Related Disease: Current and Future Insights into Pathological Diagnosis. Int J Mol Sci. 2025;26:5325. doi:10.3390/ijms26115325. URL: https://doi.org/10.3390/ijms26115325
7. IgG4ward! The Diagnostic Dilemma in IgG4-Related Disease (IgG4-RD) | Dr. Mollie Carruthers. URL: https://igg4ward.org/igg4ward-educational-resources/the-diagnostic-dilemma-in-igg4-related-disease-igg4-rd/
8. Wallace ZS, Deshpande V, Mattoo H, et al. IgG4‑Related Disease: Baseline clinical and laboratory features in 125 patients with biopsy-proven disease. (Full text via PubMed Central). 2015. URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4621270/