Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Getting the right diagnosis
Discover how doctors identify IgG4-RD using blood tests, imaging, biopsies, and clinical patterns.
 7 lessons
7 lessons Total: TBC
Total: TBC 8 minutes + video
8 minutes + videoBlood tests
Blood tests can guide care in IgG4-RD, but no single number tells the whole story.
Blood tests in IgG4‑RD: Helpful clues, not final answers
When you live with IgG4-related disease (IgG4 - RD), it’s natural to hope there’s one blood test that can say with certainty, “your disease is active” or “everything is quiet.” However, with IgG4-RD, it’s not that simple.
Because IgG4‑RD can affect different organs in each person, no single blood test works for everyone. Instead, doctors use a collection of information including your story, physical examination, imaging, blood tests, and sometimes a biopsy, to see the whole picture.
In this lesson, we’ll walk you through which blood markers often help, which don’t, and how your doctors can interpret them together over time.

Why blood tests matter, but can’t stand alone
For some diseases, the presence of a biomarker (a substance in your blood or bodily fluids that can be measured by a lab test) is a determining factor for diagnosis. This is true, for example, with some infections. But with IgG4‑RD things are a little different.
In IgG4‑RD, several biomarkers can rise during flares or settle with treatment, but they don’t do this perfectly for everyone, every time. That’s because IgG4‑RD behaves differently across people and organs. So physicians read biomarkers the way a careful detective reads clues—helpful, but only meaningful when they fit the rest of the story.
That’s why your physicians will:
Start with your symptoms and physical examination. Your lived experience guides the rest of the workup.
Add imaging when needed to see organ, swelling, or wall thickening in some structures (for example, blood vessels and bile ducts).
Use blood tests to support what they see and hear, not to replace it.
Think of blood tests as the dashboard lights in a car. They warn us to look under the hood, but they don’t fix the engine and they don’t tell us everything by themselves.
The core blood markers we follow
In IgG4-RD, there are several biomarkers in your blood that physicians track. These include:
Serum IgG4 level
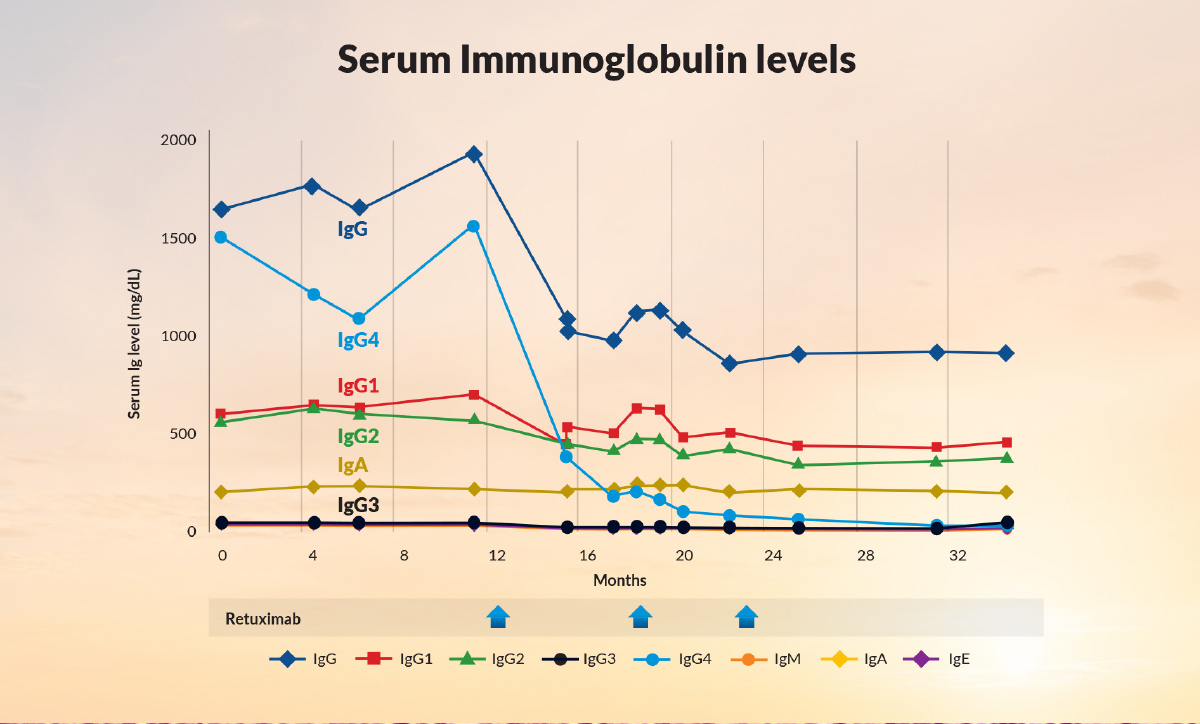
This measures the antibody called IgG4. Many—but not all—people with IgG4-RD have an elevated IgG4 at some point. In patients who start out with elevated levels, the level generally falls substantially with treatment (even though it might not become completely normal) and then rises before or during a flare. For some patients, the IgG4 level in the blood remains high after treatment but as long as the level is continuing to decline over time or is staying stable, the disease likely remains under control. In short, the TREND of serum IgG4 concentrations—whether it is increasing or decreasing from measurement to measurement—is more important than the absolute level.
Complements (C3 and C4)
Complement proteins are part of the immune system’s “first responder” team. In some people with IgG4‑RD, C3 and/or C4 run low during active inflammation. This is particularly true for patients with disease that affects many organ systems. About a third of patients with IgG4‑RD have low complement levels during periods of disease activity. Once effective treatment is given, the complement levels rise again towards normal values.
IgE, and eosinophils
IgE (an allergy‑related antibody) and eosinophils (a type of white cell) can be high in a subset of patients. These can track with flares for some people but are not specific to IgG4‑RD. The IgE and eosinophil values usually track pretty well with IgG4 levels, but in some patients IgE and eosinophil levels provide additional information about the level of disease activity.
Organ‑linked labs
Depending on where your disease lives, doctors may add targeted tests including:
› Pancreas: lipase (and sometimes amylase); can be measured in the blood. Hemoglobin A1c is another blood test that assesses patients’ recent blood sugar control. A stool sample may also be checked for an elastase level, to assess the possibility of damage to the pancreas.
› Bile ducts/liver: bilirubin and alkaline phosphatase if there is blockage or inflammation.
› Kidneys: urinalysis and urine protein (protein can be a key early clue), and creatinine to check kidney function.
Reading the numbers in real life
Blood tests help the most when we look at them over time and in context:
A sudden IgG4 spike in someone whose level usually mirrors their disease may flag a possible flare, prompting doctors to look for new symptoms or get imaging. In some cases, once doctors know a patient well, they may be comfortable adjusting treatments based on serum IgG4 levels. In general, however, IgG4 levels are used as a guide but not the sole determinant of treatment decisions.
Very high IgG4 (for example, more than five times the upper limit of normal) is strongly suggestive—but not diagnostic—because a small portion of people with other conditions (like certain diseases of the bone marrow, infections, or other immune diseases) can show big increases too.
Low complement (C3/C4) may track with activity, particularly in multi-organ disease, and can improve with treatment.
Normal labs do not rule out IgG4‑RD. Some people flare with normal IgG4 and normal complements. That ’s why your story and imaging remain central.
What blood tests can’t do
Blood tests cannot:
Diagnose IgG4-RD by themselves.
Tell us which organ is active without input from your symptoms, physical examination, and imaging.
Replace a biopsy when tissue is needed to confirm the diagnosis or rule out look ‑alikes like cancer or infection.
Putting it together: Common lab patterns by organ
Salivary/lacrimal glands: Many patients can be followed by monitoring symptoms and getting regular exams; doctors may use imaging to measure changes. Blood tests may be normal.
Pancreas and bile ducts: Imaging is key. Bilirubin and alkaline phosphatase may rise with blockage; lipase may rise with pancreatitis. IgG4 can help if it has tracked for you before.
Kidneys (tubulointerstitial nephritis): Urinalysis and protein can change before other clues; complemen ts may be low in active disease.
Aorta/retroperitoneum: Blood tests are often nonspecific here; doctors lean heavily on CT/MRI (and sometimes PET) protocols that clearly show the vessel wall and retroperitoneal tissue.
Your IgG4‑RD lab dashboard
Use this as a quick reference when you review labs with your clinician.
Marker | What it can show | What it can’t show | How we use it |
|---|---|---|---|
Serum IgG4 | May rise with flares; often falls with treatment if elevated at baseline | Doesn’t diagnose by itself; some flares occur with normal IgG4 | Track trends vs. one number; interpret alongside symptoms and imaging |
C3/C4 (complements) | Can be low in active disease, especially kidney involvement | Normal values don’t rule out activity | Helpful signal in context; follow over time |
IgE & eosinophils | May be high in allergic - leaning or active states | Not specific to IgG4‑RD | Supportive only; do not drive decisions alone |
Organ‑specific labs | Lipase (pancreas), fecal elastase (pancreas), bilirubin/alk phos (bile ducts), creatinine & urine protein (kidney) | Don’t define IgG4‑RD on their own | Guide urgency, imaging, and treatment for the affected organ |
Tip: If a lab rises, ask: Do my symptoms or images agree? Doctors rarely act on a lab result without another piece of evidence.
How often should labs be checked?
There isn’t a single rule. Your care team will personalize based on your organ pattern, your past flares, and your treatment.
Early after diagnosis or during a flare, doctors often check more frequently. About every 4 months is a reasonable rule of thumb for most patients.
If you’re stable, your doctor may stretch the interval.
When you’re approaching a time when you historically flare, your doctor may tighten monitoring for a while.
A note from the lab bench
When the lab measures IgG subclasses, it uses validated assays that separate IgG1–IgG4. Results can vary by method and lab.
Two practical take-homes:
Try to use the same lab when possible so your trends are comparable.
Ask to see both your value and the lab’s reference range; “high” or “normal” may differ slightly across labs.
What to tell your doctor so labs help you more
Bring a quick list of new or returning symptoms—even small changes, like new foamy urine, itching with jaundice, or change in dry‑gland swelling. These clues often direct the right imaging and help us interpret your labs correctly.
If a test worries you, ask, “How does this fit with my symptoms and scans?”
Summary
Blood tests are useful companions in IgG4‑RD care, but they are not the only important diagnostic tools. Serum IgG4, complements, IgE/eosinophils, and organ‑linked labs together can show patterns that align with flares or response to therapy. Doctors interpret them over time and in context, always centered on your story, physical examination, and imaging. When these pieces are combined, your doctors can make safer, more confident decisions.
References
1. Stone JH, Zen Y, Deshpande V. IgG4‑Related Disease. N Engl J Med. 2012;366:539–551. URL: https://www.nejm.org/doi/full/10.1056/NEJMra1104650
2. Peyronel F, Della‑Torre E, Maritati F, et al. IgG4‑related disease and other fibro‑inflammatory conditions. Nat Rev Rheumatol. 2025;21:275–290. URL: https://doi.org/10.1038/s41584-025-01240-x
3. Lang D, Zwerina J, Pieringer H. IgG4‑related disease: current challenges and future prospects. Ther Clin Risk Manag. 2016;12:189–199. URL: https://doi.org/10.2147/TCRM.S99985
Get the IgG4ME! app
Keep your IgG4-RD story organized in one place. Track your history, labs, and care team so you can share what matters when it matters most.
IgG4ME app