Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Getting the right diagnosis
Discover how doctors identify IgG4-RD using blood tests, imaging, biopsies, and clinical patterns.
 7 lessons
7 lessons Total: TBC
Total: TBC 8 minutes + video
8 minutes + videoClassification criteria
Learn why formal criteria exist, how they affect diagnosis of IgG4‑RD, and where they fit in the clinic and research.
How doctors classify IgG4‑related disease
When a condition can touch many organs, doctors need a shared map in order to understand what a diagnosis must consider. The classification criteria for IgG4‑related disease (IgG4‑RD) give us that map. This set of criteria does not replace a doctor’s judgment or a full diagnostic work‑up. Instead, it helps researchers and clinicians describe the same illness in the same way, so studies and treatments can move forward together.
Think of it like sorting books in a library. The labels help you find what you’re looking for, but the story still lives on the pages. In medicine, your story—your symptoms, images, lab tests, and biopsy—always comes first. The criteria help organize that story.
The classification criteria do not replace a doctor’s judgment or a full diagnostic work‑up. Instead, it helps researchers and clinicians describe the same illness in the same way, so studies and treatments can move forward together. Classification criteria are used primarily for research purposes and, indeed, have been very useful in the conduct of clinical trials in IgG4‑RD. But they are not diagnostic criteria, and some patients truly have IgG4‑RD even if they do not fulfill the classification criteria.
What “classification criteria” means
Classification criteria are rules used mainly for research. They make sure that patients enrolled in clinical trials truly share the same condition. That matters in IgG4‑RD, a disease that can look different from person to person.
Diagnostic criteria, by contrast, are meant to help a clinician decide on your individual diagnosis and care.
The American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR) have worked together to create a shared framework of classification criteria—a common “language”—that helps doctors and researchers describe IgG4-RD in a consistent way across hospitals and countries.
The current ACR/EULAR classification criteria were intentionally built to be very specific—so the people in a study truly have IgG4‑RD, even if that means some real‑world patients won’t meet them
Think of these criteria as a research checklist that helps scientists enroll the right patients, so studies are comparing the same condition. They’re designed to be very specific, which improves study accuracy, but they’re not a strict diagnostic rulebook.
There are two implications of this:
Patients enrolled in clinical studies have a high likelihood of really having IgG4‑RD (which is obviously important!)
Some patients in the “real world” may also have IgG4‑RD, even if they don’t quite fulfill the Classification Criteria.
In day-to-day care, your doctor may use the criteria as a guide, then rely on your story, physical examination, labs, and imaging to diagnose and treat IgG4‑RD even if you don’t check every box.
Classification vs. diagnosis: how clinicians actually decide
There’s no single definitive test for IgG4‑RD. Clinicians build confidence by combining your story (symptoms and exam), imaging, laboratory tests, biopsy when safe, and response to treatment.
A biopsy is the closest thing to a gold standard, but it can miss features (sampling limits, prior steroids), and some findings overlap with other diseases.
That’s why doctors use the ACR/EULAR classification rules as guideposts for including patients in trials. While diagnosis, on the other hand, remains a matter of careful clinical judgment.
The three‑step framework doctors use
Doctors assess patients based on a variety of clinical observations, symptoms, and tests. They score a patient using these criteria to assess fit for the ACR/EULAR classification.
A combined score equal or greater than 20 is used to classify IgG4‑RD.
Below 20 suggests that, for research purposes, it would be better not to include the patient in a study or trial, even if a clinician still believes the diagnosis is IgG4-RD and treats it accordingly.
1. Entry step: a typical organ or typical tissue pattern
Doctors start by asking two questions:
Is there involvement of a typical organ for IgG4‑RD (like the pancreas, bile ducts, major salivary or lacrimal glands, orbits, kidneys, lungs, aorta/retroperitoneum, pituitary, pachymeninges, or thyroid)?
Or:
Does a biopsy show a classic tissue pattern?
If one of those two things is sure, this opens the door to use the criteria.
2. Exclusion step: rule out look‑alikes
Before adding points, clinicians screen for “exclusion criteria”—features that point strongly to other conditions. These include things like blood tests strongly suggesting another disease, for example, anti‑neutrophil cytoplasmic antibodies (ANCA); the finding of “granulomas” on biopsy (granulomas, a peculiar collection of cells, suggests sarcoidosis, infection, or other diagnoses); specific tumor markers; or a clear alternative diagnosis (like lymphoma) on pathology or imaging.
A lack of response to steroids is also a red flag because most IgG4‑RD inflammation improves with steroid treatment.
Concrete mimickers to consider: sarcoidosis, ANCA-associated vasculitis (GPA), Erdheim–Chester disease, malignancy (e.g., sarcoma or lymphoma), and type 2 autoimmune pancreatitis. In a biopsy specimen, neutrophils, granulomas, and evidence of tissue death (necrosis) push clinicians toward these mimickers rather than IgG4‑RD.

3. Inclusion step: add points across eight domains
If entry is met and exclusions are absent, doctors score items across eight weighted domains. Only the highest‑scoring item in a domain counts. If the total reaches 20 points or more, a person can be classified as having IgG4-RD.
Here’s a list of those domains and why they matter:
Serology (blood tests)
A serum IgG4 level that is several times above normal adds points. High IgG4 supports the story but is never the whole story.
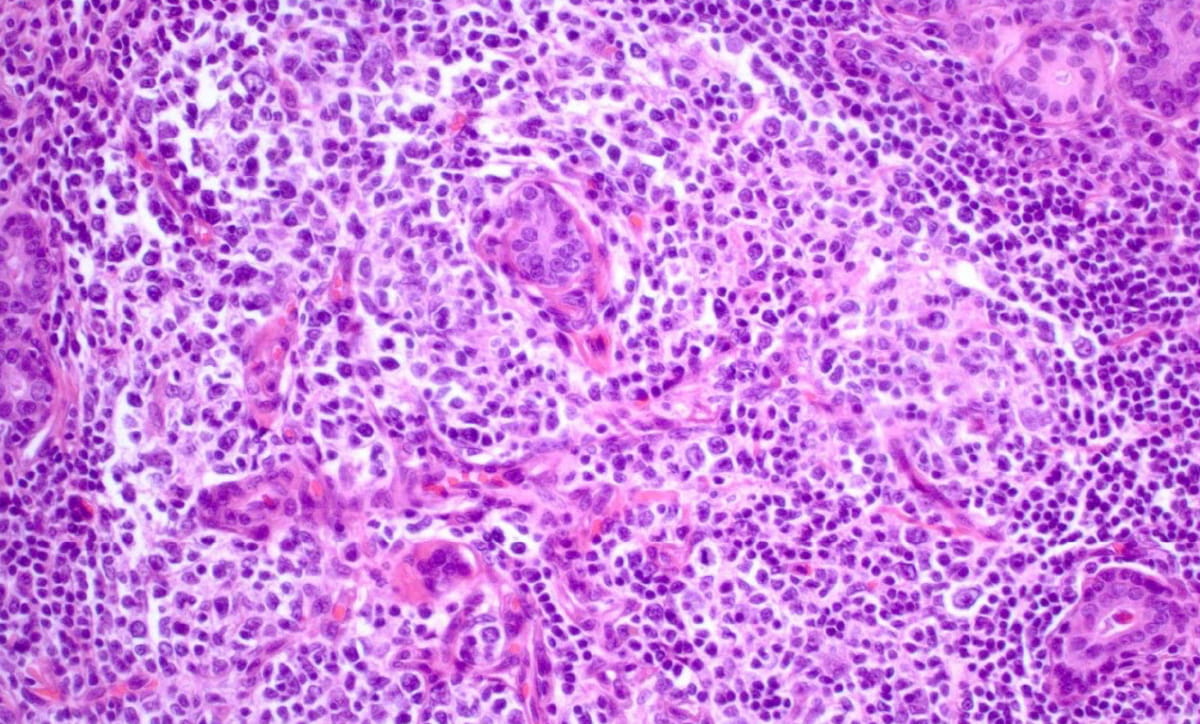
Histology (biopsy – how tissue looks under the microscope)
Certain patterns carry high weight, especially a storiform (cartwheel‑like) fibrosis pattern and obliterative phlebitis (veins damaged by inflammation). These are key signposts in many organs.
Immunostaining (IgG4 cells in tissue)
A higher IgG4+/IgG+ plasma cell ratio and higher counts per high-power field support classification. Tissue context matters; no single number is diagnostic.
Glands
Typical swelling or enlargement of the lacrimal, parotid, or submandibular glands supports classification.
Chest
Certain patterns in the chest, such as thickening of the airway walls and masses next to the spin, fitIgG4-RD more than other causes.
Pancreas and bile ducts
The combination of autoimmune pancreatitis features and bile duct strictures strongly suggests IgG4-RD.
Kidney
Findings consistent with tubulointerstitial nephritis due to IgG4-RD add points.
Retroperitoneum and aorta
Inflammation around the aorta or in the retroperitoneum (the deep space behind the abdominal cavity) can be classic for IgG4‑RD and contributes to the score.
Why doctors still look at the whole picture
The criteria are not a substitute for careful diagnosis. A few real‑world nuances:
Steroids usually help. IgG4‑RD inflammation typically responds to steroids. If a person doesn’t improve, clinicians re‑check for mimics like infection or cancer. Response itself isn’t specific—many conditions improve with steroids—so doctors use it as one clue, not the final word.
Active inflammation vs. damage. Treatments calm inflammation, but scar tissue (fibrosis) won’t shrink with immunosuppression; persistent symptoms may reflect damage rather than ongoing disease.
Some patients don’t fit neatly. People with isolated retroperitoneal fibrosis or orbital disease may have clear IgG4‑RD clinically, but not reach 20 points—especially if a safe, high‑quality biopsy is hard to obtain. Doctors consider the full context.
Serum IgG4 isn’t diagnostic. The serum IgG4 can be normal, and other antibody types can drive some features. That’s why tissue, imaging, and the clinical story are all needed.
How this helps you
For patients and families, the value of this framework is clarity. It gives clinicians shared language and thresholds when designing studies and treatments. It also helps ensure that people in a clinical trial truly have the same condition, making results more trustworthy.
At the same time, your care team will never reduce you to a number.
Doctors use the criteria as guideposts, not cutoffs. They stay focused on how you feel, how your organs are functioning, and what your tests show over time
Putting it together: a story, not just a score
Imagine two people:
One has swollen salivary and lacrimal glands, very high IgG4 levels, and a biopsy that shows storiform fibrosis. They easily pass 20 points.
Another has a single deep‑seated mass in the retroperitoneum, b iopsy is difficult, and IgG4 is only mildly elevated. Their score might be below 20, yet their doctor may still treat for IgG4‑RD if the overall picture fits.
Both deserve thoughtful care. The classification criteria organize what we see. Your clinician’s job is to interpret it with experience and compassion.
Summary
Classification criteria help us speak the same language about Ig G4‑RD, mainly for research.
The approach has three steps: entry (typical organ/pattern), exclusions (rule-outs), then inclusions scored across eight domains.
A score of 20 or more classifies IgG4‑RD, but some true cases won’t reach that bar.
Doctors combine the score with your biopsy, imaging, blood tests, and response to treatment to make the best decision for you.
References
Stone JH, Zen Y, Deshpande V. IgG4-Related Disease. NEJM. 2012;366:539–551. URL: https://www.nejm.org/doi/full/10.1056/NEJMra1104650
Peyronel F, Della-Torre E, Maritati F, et al. IgG4-related disease and other fibro-inflammatory conditions. Nat Rev Rheumatol. 2025;21:275–290. URL: https://doi.org/10.1038/s41584-025-01240-x
Lang D, Zwerina J, Pieringer H. IgG4-related disease: current challenges and future prospects. Ther Clin Risk Manag. 2016;12:189–199. URL: https://doi.org/10.2147/TCRM.S99985
Get the IgG4ME! app
Keep your IgG4-RD story organized in one place. Track your history, labs, and care team so you can share what matters when it matters most.
IgG4ME app