Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Treatment and disease management
Understand how inflammation is managed through steroids, immune therapies, and supportive care—and what to expect at each step.
 8 lessons
8 lessons Total: tbc
Total: tbc 12 minutes + video
12 minutes + videoB‑cell depletion
Learn why B cells are targeted in IgG4-RD, how rituximab and inebilizumab work, and how response is tracked.
Putting out the fire: How B-cell depletion helps calm IgG4‑related disease
When you’re facing IgG4‑related disease (IgG4‑RD), it helps to understand why some treatments focus on depletion of a group of immune cells called B cells.
As you’ve seen, B cells are the team’s “memory keepers” and antibody makers. In IgG4‑RD, parts of this team become overly active and noisy, sending signals that keep inflammation smoldering. B-cell depletion is a way of turning down that noise so your organs can heal.
This lesson explains, in clear, practical terms, why B-cell–targeted therapy helps many people with IgG4-related disease (IgG4-RD), what the treatments are, how they’re given, what to expect, and how your team monitors safety and response.
What do we mean by B-cell depletion?
B cell depletion means giving a treatment to lower certain immune cells (B cells) temporarily. B cells are one of the key drivers of IgG4-RD, a type of cell that keeps the inflammation “conversation” going in IgG4‑RD. By removing these upstream cells, a lot of important signals downstream are also diminished. The results: a quieter the immune system, a reduction in swelling and pain, and an opportunity for the organs affected by IgG4-RD to heal. More mature cells such as the plasma cells are not affected by B cell depletion so the patient retains the capacity to make the antibodies that he/she already makes, but the fuel for ongoing inflammation is reduced.
Rituximab (anti-CD20)
The best‑known medication for B-cell depletion is rituximab. Rituximab is itself an antibody that recognizes a protein called CD20, which is present on the surfaces of most B cells. Rituximab, which is administered by infusion (through an IV in the patient’s arm), lowers the B cells that feed the inflammatory loops of IgG4-RD. By pressing “pause” on these upstream cells, the downstream signals quiet, disease activity falls, serum IgG4 levels decline, and IgG4-RD patients feel better.
Inebilizumab (anti-CD19)
Another medication for B-cell depletion is inebilizumab, another antibody that targets a different protein on the surfaces of B cells, CD19. Inebilizumab was tested in a worldwide clinical trial of patients with IgG4-RD known as the MITIGATE trial, and it has been approved by the FDA specifically for the treatment of IgG4-RD. (In contrast, rituximab is not an approved medication, though it is sometimes used “off-label’). Infliximab is administered as an infusion, as well. Inebilizumab (brand name Uplizna) was approved by the U.S. Food & Drug Administration (FDA) in April of 2025, and has now been approved in the European Union, the United Kingdom, Canada, Japan, China and many other countries throughout the world. The worldwide approval of inebilizumab reflects the growing international recognition that targeting B cells (including CD19+ B-cell lineages) can help prevent flares and support long-term disease control.
How B cell depletion works
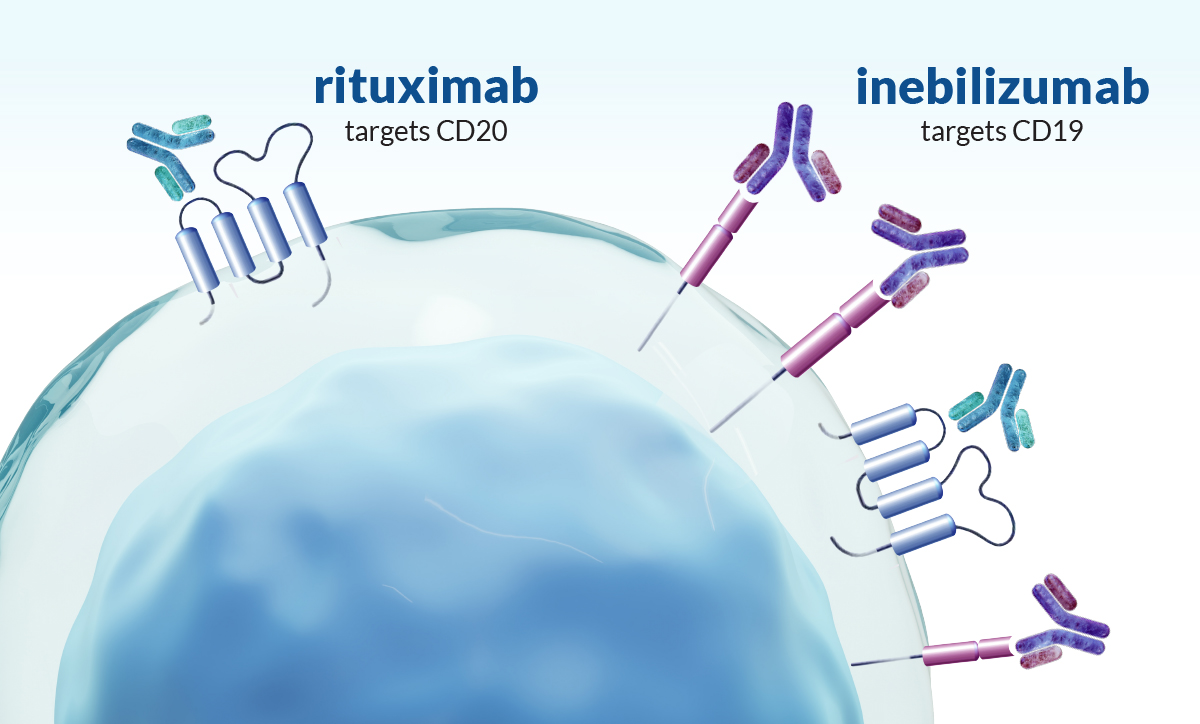
B cell–depleting medicines: rituximab (targets CD20) and inebilizumab (targets CD19), bind markers on B cells so your body clears these cells from circulation for months.
Clinicians describe this as “resting” the B‑cell part of the immune system. Because the short‑lived cells that drive IgG4‑RD rely on a steady supply of new B cells, removing that supply quiets the immune “chatter,” and lets inflamed tissues heal.
Many people notice improvement within weeks. They experience a reduction in swelling and pain, and more energy, although timing varies by person and organ.
B cell depletion options at a glance: rituximab vs. inebilizumab
Treatment | Antibody target | FDA approval for IgG4-RD (US) | Typical dosing schedule | When to consider it |
|---|---|---|---|---|
Rituximab | CD20 on mature B cells | Not FDA‑approved for IgG4‑RD (commonly used off‑label)1 | Commonly 2 IV infusions given 2 weeks apart for induction; maintenance varies by center and patient 2,3 | Broad clinical experience; useful when rapid disease control is needed, prior good response to rituximab, or access/coverage favors rituximab1 |
Inebilizumab | CD19 (broader B cell lineage) | FDA‑approved for adults with IgG4‑RD (2025) 4 | 2 startup infusions (Day 1 and Day 15), then one infusion every 6 months 5,6 | On‑label option; consider when a labeled therapy is preferred, for broader B cell lineage depletion, for scheduled every 6‑month maintenance, or after inadequate durability/ tolerance with rituximab 4,7 |
Clinical decision‑making is individualized; safety screening (e.g., hepatitis B), vaccine timing, infection monitoring, and infusion‑center administration apply to both.
What MITIGATE taught us about B cell–directed therapy
To understand why B‑cell–directed therapy matters, it helps to look at MITIGATE, a 52‑week, global, randomized trial that compared inebilizumab (targets CD19 on B cells) with placebo. All patients in the trial started with a short steroid taper, then the study measured how many people stayed in remission without going back on steroids. [1]
Here’s the heart of it: People on inebilizumab were far less likely to flare: an 87% reduction in flare risk over the year. About 90% of patients on inebilizumab were able to come off steroids and stay off, compared with about 37% on placebo with the short taper. Serious side effects happened in both groups and were tracked closely. [1]
Bottom line: B‑cell–directed therapy can keep disease quiet while helping many people avoid the long‑term downsides of steroids. Your plan is still tailored to you. It is based on which organs are involved, your past responses, and your health history. [1]
Key outcomes from the MITIGATE clinical trial
Outcome (52 Weeks) | Inebilizumab | Placebo/ Prednisone | What It Means |
|---|---|---|---|
Risk of Flare | ↓87% reduction of disease flare vs placebo) | — | Flares were much less likely with inebilizumab. |
Off‑Steroid Remission | ~90% remained off steroids | ~37% | Most patients avoided going back on prednisone with inebilizumab. |
Serious Adverse Events | ~18% | ~9% | Serious events occurred in both groups but a higher number were observed in the inebilizumab group; infections and hospitalizations were tracked closely. |
Takeaway: B cell–directed therapy can keep disease quiet and reduce steroid exposure for many. (We still individualize choices based on your organs involved, prior treatments, and risk factors.)
What to expect from treatment
How it’s given
B cell–depleting therapy is delivered by IV in an infusion center. Two medicines are commonly used in IgG4-RD care: rituximab (targets CD20 on B cells) and inebilizumab (targets CD19, which is found on a broader range of B-cell stages, therefore theoretically leading to higher efficacy). Both are given as monitored infusions; the exact schedule varies by center and by your situation.
A common induction plan with both of these medications involves two infusions two weeks apart, with some centers repeating infusions later to maintain remission. Your team will tailor timing to disease activity, organs involved, prior medicines, and how you respond.
Why infusion centers
Infusions are done in staffed centers so nurses and clinicians can manage reactions immediately (for example, slowing the rate or giving medicines on the spot).
Before each infusion
You’ll typically have blood tests and a check‑in about infections, vaccines, and medicines. Pre‑medications (like acetaminophen, an antihistamine, and sometimes methylprednisolone, a steroid) help reduce infusion reactions.
During and after
Infusions are monitored carefully. Some of the most important potential side effects, though relatively rare, pertain to the time when the drug is being administered. After the infusion is done, the risk of those adverse effects subsides. Patients are typically observed for one hour after an infusion.
If reactions happen, they’re usually mild (feverish feeling, flushing, itching) and improve with rate adjustments or medications. Over days to weeks, many people notice less swelling or pain, and lab markers improve over time. Your team may follow serum IgG4 and other labs, along with how you feel and imaging when needed.
Benefits and limitations
Most people with active IgG4‑RD improve with B-cell depletion, especially when inflammation is the main driver. When advanced fibrosis (scar tissue) is present, responses can be less complete. That’s because scar tissue doesn’t resolve quickly. Even then, reducing inflammation may still prevent new damage. Your clinician will balance urgency, organ risk, and the likelihood of benefit when recommending therapy.
When to treat versus monitor: what clinicians consider
Not every patient must be treated immediately
IgG4 specialists have noted that a small subset of patients (often those with head and neck–predominant disease such as isolated, painless submandibular or parotid gland enlargement) may be observed over time if symptoms are minimal and the patient prefers watchful waiting. Even then, careful follow‑up is essential because silent disease in other organs is possible.
Look for hidden involvement
When only one area seems involved, physicians typically screen for other organ disease with imaging. This may include: CT of the chest, abdomen, and pelvis, and head/neck when appropriate, plus labs and a thorough physical examination.
If the serum IgG4 is very high (for example, ~1,500 mg/dL), isolated salivary disease is unlikely, and physicians may assume additional involvement until proven otherwise; in such cases, physicians will generally treat with medication.
Studies show that patients on average have about three organs involved at diagnosis. [12]
Why treatment is recommended
Unchecked inflammation can cause organ dysfunction over time. For kidneys, pancreas, lungs, or other critical organs, clinicians may prefer timely therapy rather than prolonged observation, aiming to “put the fire out” before lasting damage accrues.

Vaccination before treatment is important
Because rituximab reduces B cells, your body may not respond as strongly to vaccines right after treatment. When possible, vaccines are best given 3-4 weeks before starting therapy, so you can build protection first. [8]
Age‑ and risk‑appropriate vaccines include:
COVID‑19 (mRNA), influenza (yearly), pneumococcal, shingles (recombinant zoster, 2‑dose series), and RSV when eligible.
While B cells are depleted, vaccine responses can be weaker. Some clinicians give boosters as B cells recover between cycles. Household members staying up to date adds a layer of protection for you. Live vaccines are usually avoided during significant immunosuppression.
Tip: Consider using the IgG4ME! app to keep track of your vaccine history and timing.
IgG4ME appPractical takeaways:
If possible, get needed vaccines before starting B-cell–depleting therapy.
If you’re already on treatment: non-live vaccines are generally safe but may work less well; timing may be adjusted to when B cells begin to return.
Avoid live vaccines during significant immunosuppression.
Keep household members up to date on vaccines.
Get our vaccination guide
Review these vaccine recommendations before you begin treatment
Missing PDF and linkMore vaccine information to review
You may wish to review these two videos from the IgG4ward! Resource Center with discussions about vaccines before treatment. (See the “Related Resources” section at the end of this lesson).
Fireside Chat: IgG4-RD & Vaccines – Community Q&A (Dr. Stone and Dr. Kotton) https://igg4ward.org/igg4ward-educational-resources/fireside-chat-igg4-rd-vaccines/
Good Question Series: Special Edition – Vaccine Follow-up Questions (Dr. Stone) https://igg4ward.org/igg4ward-educational-resources/igg4rd-vaccine-questions/
Safety notes you should know
All medicines have risks. For rituximab and inebilizumab, the main concerns are infusion reactions and infections.
infusion reactions (early) and serum sickness (delayed, rare): Most infusion reactions are manageable in the treatment center. Rarely, anaphylaxis can occur during an infusion. Serum sickness (a delayed immune‑complex reaction) is also rare but recognized. These risks are why infusions happen where trained staff can act immediately. [2, 10]
Hepatitis b reactivation: Screen and prevent. Before starting therapy, teams screen everyone for prior hepatitis B exposure (HBsAg and anti‑HBc). If prior exposure is found, starting antiviral prophylaxis and continuing it through B‑cell depletion (and for a period afterward) can prevent reactivation. [2]
Shingles (herpes zoster): Prevention matters. Shingles can be a problem after B‑cell depletion but is largely preventable when vaccinated beforehand with the recombinant zoster vaccine. [9]
Hypogammaglobulinemia: Some people, especially with repeated courses, develop low immunoglobulin levels. If levels fall and infections recur, your team may recommend IVIG replacement. [11]
infection risk beyond antibody levels: Even apart from low immunoglobulins, being B‑cell depleted increases infection risk. Hand hygiene, staying current with vaccines, and alerting your team to fevers or new symptoms are important. [2, 11]
Neutropenia: A low white blood cell count can occur after B‑cell depletion; clinicians monitor counts and treat as needed. [2]
Dr. Stone discusses how to avoid side effects from B-cell depletion treatments.
Patient safety: What we do to make infusion treatment safer
Screen for hepatitis B; give antiviral prophylaxis if prior exposure is present.
Vaccinate before treatment when possible (COVID‑19, flu, pneumococcal, shingles, RSV).
Premedicate and infuse in a center prepared to treat reactions immediately.
Monitor immunoglobulin levels and white blood cell counts; consider IVIG if infections recur with low Ig levels.
Plan timing for boosters as B cells recover.
Steroids and combination therapy: Why your plan may include both
Steroids are typically started first
Many people start treatment for IgG4‑RD with glucocorticoids (steroids) because they work quickly. Rituximab or inebilizumab is often added to help control disease long‑term and reduce steroid exposure. In some situations, like when steroids are poorly tolerated or not advised, B cell depletion can serve as a primary therapy.
Short courses with a purpose
When the decision to deplete B cells is uncertain, such as mild, localized disease, clinicians may use a brief prednisone course (for example, ~2 months then stop). If improvement is dramatic and sustained, some patients can remain off additional therapy with close monitoring. If disease recurs or multiple organs are at risk, we move on to B cell–targeted therapy sooner.
Limits of conventional steroid‑sparing drugs
Traditional csDMARDs (such as methotrexate, azathioprine, mycophenolate) have mixed and mostly anecdotal support in IgG4‑RD. They may seem to help while steroids are on board, but relapses often emerge when steroids stop. Because active disease can be hard to detect early, relying on csDMARDs alone can risk silent progression. For many patients needing more than steroids, rituximab is preferred to fully extinguish inflammation. [2]
Personalized support on your steroid journey
Get support and education on your steroid journey with a new digital companion, Sam (Steroids and Me). Find answers and learn how to work with your doctors for the best care and taper plan.
GET SAM NOWA patient story
William Joy lived for years with swollen salivary (parotid) glands. After B-cell depletion with rituximab, the swelling eased quickly, his energy improved, and his blood tests trended back toward normal.
His experience helped show doctors treating patients with IgG4-RD that targeting upstream B cells can quiet IgG4-RD fast, reduce steroid needs, and lower flare risk. This helped in guiding clinicians to tailor treatment to the organs involved and each person’s goals.
Randomized trial data have since reinforced that B‑cell–directed therapy significantly lowers flare risk and reduces steroid exposure, aligning with what many patients feel day to day.
It’s important to keep in mind, however, that every person’s course is different. That is why physicians plan care around which organs are involved while taking into account each person’s risks and goals.
Looking ahead: therapies on the horizon
Scientists are exploring new ways to calm the overactive B cells that help drive IgG4-RD. Some up-and-coming therapies include:
Obexelimab (CD19-Targeted B-Cell Modulator)
This drug “turns down” B-cell activity rather than fully depleting cells to help quiet inflammation. A phase 3 clinical trial of obexelimab has been completed, but obexelimab is not yet available for clinical use.
BTK Inhibitors (such as Rilzabrutinib; Oral Pills)
These medications block B-cell signaling pathways to reduce flares and symptoms, aiming for fewer side effects. BTK inhibitors are in clinical testing for IgG4-RD and are therefore still investigational.
Cell-Based Therapies (Early-Stage: CAR-T, CAR-NK, Gamma-Delta T-Cell Platforms)
Engineered immune cells designed to target the same B-cell markers as rituximab and deliver effects directly in tissues.
These therapies remain investigational at this time. These therapies on the horizon are experimental and only available in clinical trials right now.
Talk with your specialist to review risks, benefits, and eligibility.
Questions patients often ask
How long does it last? B cells usually begin to return over several months. Some people stay well without more treatment; others need maintenance doses.
Will B-cell depletion cure IgG4‑RD? It’s not a cure, but it can bring remission—a quiet state where symptoms and inflammation are controlled—often with fewer steroids.
Can I work and exercise? Most people can continue daily life, adjusting for infusion days and how they feel. Gentle activity is encouraged; your team can tailor guidance to your organs involved.
What if I relapse? Relapses can happen. If they do, your team may repeat rituximab, adjust medicines, or reassess the diagnosis and organ status.
Summary
B cell depletion with rituximab aims to calm the over‑active parts of the immune safety team in IgG4‑RD. It often works quickly on inflammation, may help protect organs from further damage, and can lower the need for long‑term steroids.
Planning around vaccines and monitoring for infections keeps treatment safer. When scarring is advanced, improvement may be more modest, but controlling ongoing inflammation still matters.
Every individual’s care plan is personalized. Your clinicians will work closely with you to determine the best course of treatment.
References
1. Tanaka Y, et al. Perspectives on current and emerging therapies for IgG4-related disease. Mod Rheumatol. 2023;33(2):229–241.
2. Rituximab (Rituxan) Prescribing Information. U.S. FDA; updated 2021.
3. Majumder S, et al. Rituximab Maintenance Therapy Reduces Rate of Relapse in IgG4-Related Disease. Clin Gastroenterol Hepatol. 2018.
4. Amgen. UPLIZNA (inebilizumab-cdon) FDA approval for IgG4-RD. Press release; April 3, 2025.
5. UPLIZNA HCP – Infusion Guide. Day 1/Day 15, then q6 months; pre-med/monitoring.
6. UPLIZNA Patient – Dosing/“How to take”. Maintenance every 6 months.
7. Stone JH, et al. Inebilizumab for Treatment of IgG4-Related Disease (MITIGATE). N Engl J Med. 2025.
8. Bass AR, Chakravarty E, Akl EA, et al. 2022 ACR Guideline for Vaccinations in RMD. Arthritis Care Res (Hoboken). 2023;75(5):e97–e114.
9. Anderson TC, et al. Recombinant Zoster Vaccine in Immunocompromised Adults ≥19 Years—ACIP, 2022. MMWR. 2022;71:80–84.
10. Bayer G, et al. Rituximab-induced serum sickness is more frequent in autoimmune diseases. Autoimmun Rev. 2019.
11. Tieu J, et al. Rituximab-Associated Hypogammaglobulinemia in Autoimmune Disease. Front Immunol. 2021.
12. Yamada K, Yamamoto M, Saeki T, et al. Arthritis Research & Therapy. 2017.
13. Stone JH, Zen Y, Deshpande V. IgG4-Related Disease. N Engl J Med. 2012;366:539–551.
Personalized support on your steroid journey
Get support and education on your steroid journey with a new digital companion, Sam (Steroids and Me). Find answers and learn how to work with your doctors for the best care and taper plan.
Get SAM Now