Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Understanding the disease
What IgG4-related disease is, why it can look like many other conditions, and how it affects the body.
 8 lessons
8 lessons Total: TBC
Total: TBC 7 minutes + video
7 minutes + videoThe role of B cells and why they matter
Meet the immune cells at the center of IgG4-RD, and learn how B cells drive IgG4, inflammation and fibrosis.
What are B cells and why they matter
B cells are white blood cells that specialize in making antibodies: the Y‑shaped proteins that tag germs so the rest of your immune system can clear them. Think of B cells as one part of your body’s safety team. In IgG4‑related disease (IgG4‑RD), some B cells and their descendants become over‑helpful and confused.
This lesson explains what B cells do in healthy immunity, what changes in IgG4‑RD, and why many treatments focus on calming B cells down.
B cells at a glance
B cells are antibody makers. They help you fight infections by making proteins called antibodies.
In IgG4‑RD, certain B cells become overactive. They mature into plasmablasts and plasma cells that can make large amounts of antibodies, including IgG4.
B cells don’t act alone. Special T cells “coach” B cells; together they can drive inflammation and fibrosis (scarring) in affected organs.
Treatments that reduce B cells (like anti‑CD20 or anti‑CD19 medicines) often quiet disease activity.
B cells in over-drive
B cells start their training in the bone marrow, rotate through the lymph nodes and spleen, and, with coaching from helper T cells, “graduate” into specialists:
plasmablasts (short‑lived sprinters that make lots of antibody quickly)
plasma cells (long‑lived marathoners that keep protective antibody levels steady)
memory B cells (a few specialize this way), so you can respond faster the next time an infection shows up
In IgG4‑related disease (IgG4‑RD), some members of this safety team become over‑helpful and confused. Signals from T cells push B cells to switch toward making IgG4 antibodies. Plasmablasts expand in the blood and plasma cells collect in tissues. The constant “chatter” between B and T cells draws in more immune cells and fibroblasts, which can lead to inflammation and scarring (fibrosis) in affected organs.
Plasma cells are what B cells evolve into at the conclusion of their development.
That’s why many effective treatments aim to quiet B cells—by reducing their numbers or dialing down their activation. When B cells settle, the whole inflammatory loop calms, symptoms improve, and organs have a chance to heal.
Meet the B cell
What is a B cell?
The B cell is a white blood cell that learns to recognize germs and makes antibodies to stop them. B cells start in the bone marrow, then travel to lymph nodes and the spleen where they continue their education.
You can think of B cells as having life stages:
Early B cell (in bone marrow) — learning the basics.
Mature naive B cell (in lymph nodes/blood) — a rookie that hasn’t seen its first “assignment” yet.
Activated B cell — meets a target and gets help from T cells; starts changing.
Plasmablast — the sprinting phase: travels in blood and makes lots of antibodies.
Plasma cell — the marathoner: settles mainly in bone marrow and keeps making antibodies for a long time.
What CD markers mean
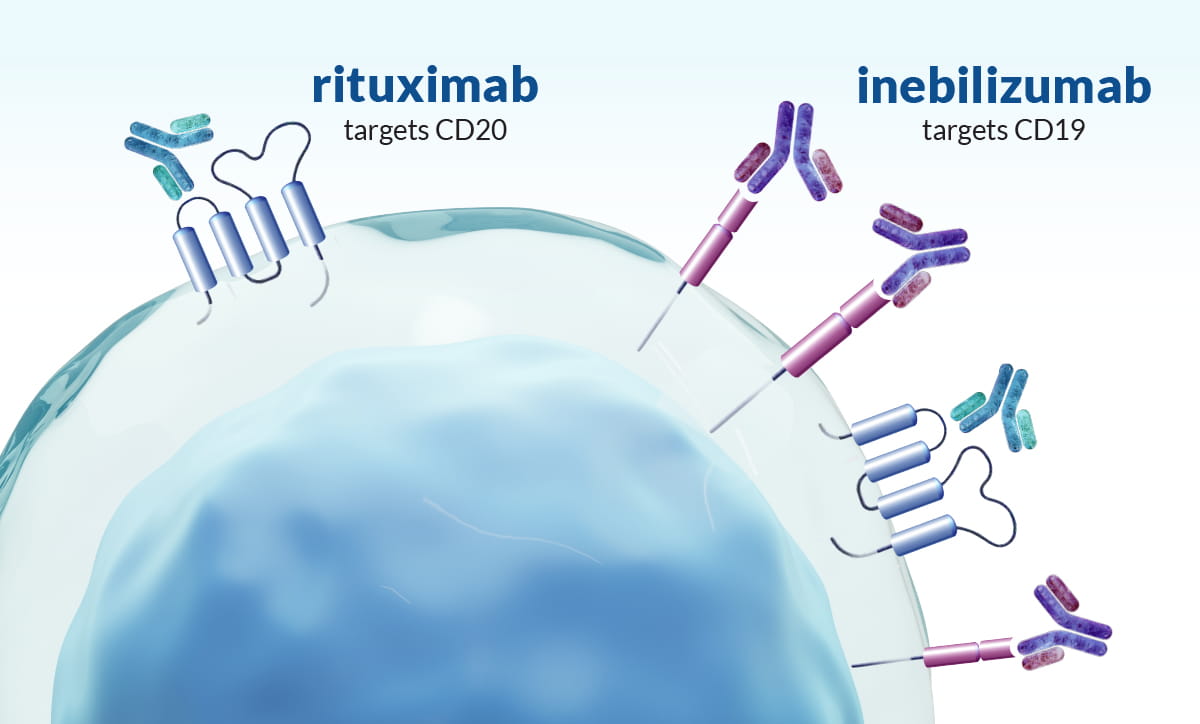
B cells carry “name tags” on their surface. Two common tags, or markers are CD19 and CD20.
“CD” stands for cluster of differentiation—standard names for proteins on a cell’s surface. Think of them like uniform badges scientists use to tell immune cells apart and to guide certain medicines.
Most B cells have both CD19 and CD20 markers, but plasmablasts often lose CD20 and keep CD19. This matters because some therapies can find and calm B cells by targeting these markers.
Changes in IgG4‑RD
In IgG4‑RD, the immune system becomes over‑revved in certain places (like the pancreas, salivary glands, kidneys, or around big blood vessels). Several things happen together:
Extra‑helpful B cells expand. You may see more plasmablasts in the bloodstream. These cells can make antibodies quickly, including IgG4, and can collect in tissues.
Coaching from T cells increases. Special T cells (sometimes called T follicular helper cells) encourage B cells to “class‑switch” and make more IgG4. Other T cells can release proteins that attract scar‑forming cells (fibroblasts), leading to fibrosis.
Tissue becomes crowded. Many B cells, plasma cells, and T cells move into the affected organ. Over time this can create firm, mass‑like swelling and scarring if not treated.
Why IgG4?
IgG4 is one of the body’s four IgG subclasses. In healthy systems, it often shows up after long‑term exposures (like allergies or chronic stimulation). In IgG4‑RD, signals from T cells and B cells push more production of IgG4 than usual. IgG4 itself may not be the only driver of disease, but it is a useful clue for doctors and part of the bigger immune picture.
How B cells contribute to inflammation and fibrosis
Think of a feedback loop:
B and T cells talk a lot. T cells provide “help” signals (chemical messages) that tell B cells to grow and switch to making IgG4.
Plasmablasts and plasma cells accumulate. They make antibodies and also release messengers that keep immune cells coming.
Fibroblasts are called in. These cells lay down collagen — the “building material” of scar tissue. Over time, this can lead to storiform fibrosis (a whorled pattern of scarring that pathologists see under the microscope).
Blood vessels can be affected. In some tissues, small veins can get inflamed (obliterative phlebitis). Together, these changes create the classic tissue pattern of IgG4‑RD.
The good news: because B cells sit near the “start” of this loop, calming or reducing B cells can quiet the whole process.
Why B‑cell‑targeted treatments help
Anti‑CD20 therapy (e.g., rituximab) — reduces many B cells that carry CD20. This often lowers plasmablast levels and improves symptoms.
Anti‑CD19 therapy (e.g., inebilizumab) — can reach even earlier B cells (and many plasmablasts), sometimes leading to a deeper or longer response.
Why don’t we remove plasma cells directly?
Long‑lived plasma cells (the marathoners) often lack CD20 and may sit safely in the bone marrow. They are harder to target. But if we shrink the pool of earlier B cells and plasmablasts, the fuel for inflammation drops, and tissues get a chance to heal.
Lowering B cells can raise infection risk for a while. Your care team may time any vaccines, check blood counts, and watch for signs of infection. Most people do well with careful monitoring.
What this means for patients
If IgG4 level is high or biopsy shows many IgG4‑positive plasma cells, that is just one part of the diagnosis puzzle.
Not everyone with IgG4‑RD has the same organs involved. The pattern varies; treatment is tailored to each patient.
B‑cell‑focused therapies can be powerful tools to control inflammation and prevent scarring.
Summary
B cells are essential defenders. In IgG4‑RD, certain B cells and their partners get stuck in “overdrive,” sending too many antibody‑making cells into tissues and encouraging scarring. Because B cells help start this chain reaction, treatments that calm or reduce B cells often bring relief and protect organs. With monitoring and a personalized plan, most people do well.
A glossary of common terms
Antibody: A protein that recognizes a target (like a virus) to help neutralize it.
Class‑switching: When a B cell changes the type of antibody it makes (for example, switching to IgG4).
Plasmablast: A fast‑moving, short‑lived antibody‑making cell in the blood.
Plasma cell: A long‑lived antibody‑making cell that often resides in bone marrow.
Fibrosis: Build‑up of scar‑like tissue that can stiffen organs.