Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Understanding the disease
What IgG4-related disease is, why it can look like many other conditions, and how it affects the body.
 8 lessons
8 lessons Total: TBC
Total: TBC 10 minutes
10 minutes Other important immune cells
Meet other players in IgG4-RD that influence scarring and treatment: T cells, eosinophils, and fibroblasts.
The supporting cast that drives inflammation — and healing
Beyond B Cells: How T cells, Eosinophils, and Fibroblasts Shape IgG4-RD
When you hear “immune system,” you might think of antibodies and B cells. In IgG4‑RD, B cells are important—but they don’t act alone.
This lesson introduces three other players that shape inflammation and scarring: T cells, eosinophils, and fibroblasts. Understanding how they talk to B cells—and to each other—helps explain why tissues swell and stiffen, and why certain treatments help.
Let’s get started.
A quick look at the main players
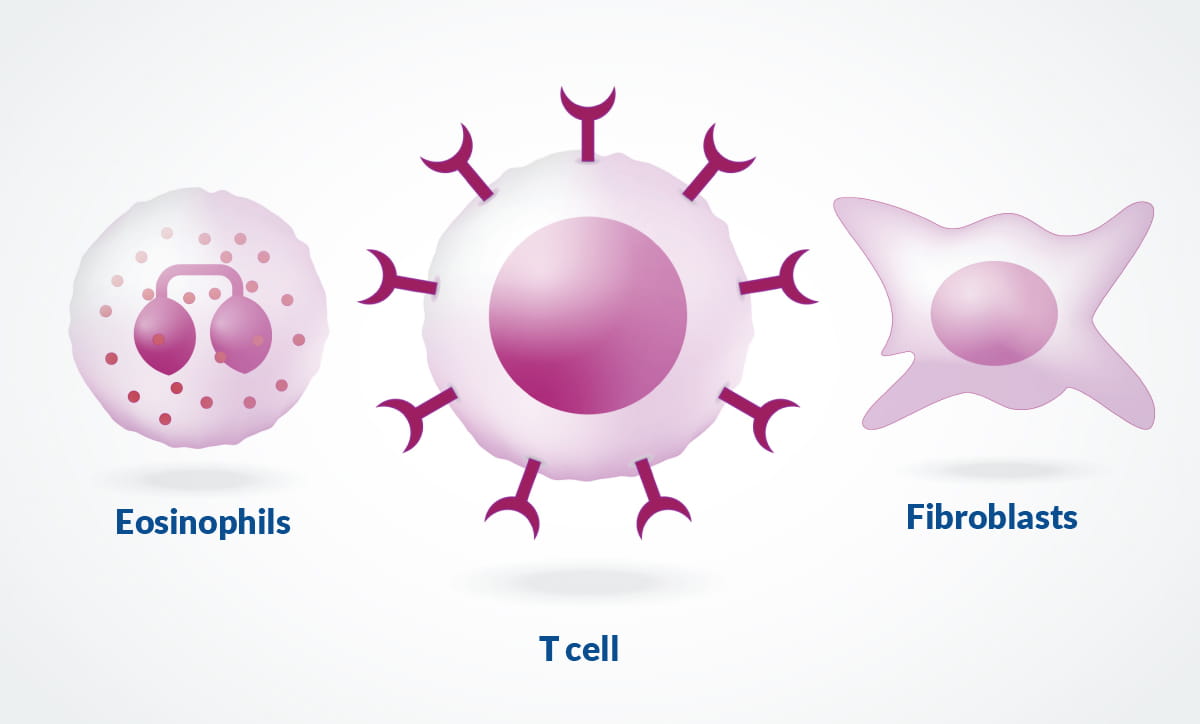
Beyond B cells, three other types of cells play a key role in IgG4-related disease. Imagine a neighborhood watch: some neighbors coordinate, some call in reinforcements, and some bring tools to fix what’s broken. Understanding each of their roles in IgG4‑RD can help you understand what comes next.
T cells: The immune system’s coaches and coordinators. They guide other cells (like B cells) and, if overactive, can mistakenly inflame or damage healthy tissue.
Eosinophils: Allergy-linked white blood cells that release chemicals and cytokines (chemical messengers). In excess, they can add to swelling, pain, and irritation.
Fibroblasts: The body’s repair crews that lay down collagen after injury. When overstimulated, they overbuild, leading to fibrosis (scar-like tissue).
Meet the cells
T cells: The coaches and coordinators
Let’s start with T cells—the coordinators. When IgG4‑RD is active, these cells set the tone for the whole response, telling B cells what kind of antibodies to make and nudging repair crews (fibroblasts) to work faster. Different T cell subtypes play different parts:
Helper T cells (Th)
Th2 cells promote IgG4 and IgE responses by releasing signals like IL‑4 and IL‑13. This can tie IgG4‑RD to allergy‑type features in some patients.
T Follicular Helper (Tfh) cells live near B cells and help them mature. Tfh2 cells help B cells switch to making IgG4 antibodies, while Tfh1 cells can promote IgG1 and other complement-activating antibodies in certain IgG4-RD phenotypes.¹
Think of T follicular helper (Tfh) cells as coaches who sit right beside B cells in the lymph nodes and help them “graduate.” Part of that coaching is helping B cells switch classes—basically swapping to the antibody type that best fits the job.
Tfh2 coaches tend to guide B cells to make IgG4, a type that usually keeps the inflammatory “alarm system” quieter. Tfh1 coaches more often steer B cells toward IgG1, which can flip on complement—a protein alarm system that ramps up inflammation. Different patients can lean more toward one pattern or the other, which is what we mean by “certain phenotypes.”
Regulatory T cells (Tregs)
Think of Tregs as peacekeepers that release calming signals—one is IL-10, a “slow-down” message for the immune system. In IgG4-RD, there can be more Tregs, and their IL-10 can nudge B cells toward making IgG4 antibodies, yet they don’t completely turn off the inflammation. So you get a “quieter but persistent” response that still causes problems.
Cytotoxic T cells (CD4+ and CD8+)
These are the immune system’s demolition team. In IgG4-RD, a notable subset of CD4 cytotoxic T cells gathers in affected tissues and releases cell-injuring proteins and alerts that call in fibroblasts. Fibroblasts then lay down extra collagen, setting the stage for fibrosis (scar-like thickening).²
What it means clinically
Different organs tend to flare when different T cell “teams” take the lead. In the head and neck glands, helper types like Th2/Tfh2 are often in charge; around the aorta and in the retroperitoneum, the cytotoxic T cells usually drive the action.
Doctors use this insight to choose treatments that fit the biology, such as using targeted medicines to calm B cells or using steroid-sparing options when possible.
Eosinophils: The allergy link
If T cells are the coordinators, eosinophils are the strong‑armed helpers who show up when allergy signals blare. Many patients never notice them; others—especially with asthma, eczema, or seasonal allergies—see eosinophils join the scene.
Eosinophils are common in people with asthma, eczema, or seasonal allergies, and can be seen in some IgG4‑RD tissues and blood tests.¹–²
They release granules and cytokines that add to swelling and tissue irritation. This can worsen gland swelling, sinus issues, or lung symptoms in some patients.
Elevated eosinophil counts or IgE can nudge clinicians to look for allergy‑associated phenotypes of IgG4‑RD and monitor for organ involvement.¹-²
Eosinophils don’t cause IgG4‑RD by themselves, but they can amplify inflammation and symptoms in certain patients.
What it means clinically
When a patient’s history suggests allergies, such as asthma, eczema, or seasonal allergies, clinicians often check a complete blood count for eosinophils and measure IgE. If either is elevated, it nudges the team to look more closely for involvement of tissues that tend to be reactive in this setting, such as the sinuses, airways/lungs, and salivary glands, and to correlate with imaging or biopsy when appropriate.
Keep in mind that eosinophils are amplifiers, not the root cause of IgG4-RD. Their presence helps clinicians phenotype the disease (allergy-associated vs. not) and tailor monitoring and counseling, but they don’t define the diagnosis by themselves.
Fibroblasts: From repair to scar (fibrosis)
Meet the builders. Fibroblasts are the body’s repair crews—essential after any injury. The issue in IgG4‑RD isn’t that they’re present; it’s that the repair orders can become too loud and too long‑lasting.
Fibroblasts are normal “repair crews” that lay collagen after injury.
In IgG4‑RD, immune signals (from T cells and others) can switch fibroblasts into overdrive, creating the classic storiform (whorled) fibrosis seen on biopsy.
Too much fibrosis can narrow ducts or squeeze organs—causing jaundice (bile duct compression), kidney problems (ureteral compression), or orbital swelling around the eyes.
What it means clinically
When fibroblasts shift into “overdrive,” the main risks are blockages and pressure effects on nearby structures. Clinicians watch for warning signs tied to where fibrosis forms—for example, painless jaundice or itching if the bile duct is squeezed, flank pain or rising creatinine if the ureter is narrowed, or eyelid/orbital fullness and vision changes around the eyes.
Imaging (ultrasound, CT, or MRI) helps spot thickening and narrowing, while biopsy—when safe—confirms the pattern of storiform fibrosis and rules out mimics. Early treatment matters because newer fibrosis can soften or regress, while long-standing scar is harder to reverse.
Steroids and B‑cell–targeted therapies can quiet the signals that drive fibroblasts.
How these cells talk to each other
Here’s the typical storyline. A trigger flips the switch in a tissue, T cells start giving directions, and others follow. Without treatment, the conversation loops and gets louder over time.
Trigger (unknown in many cases) leads to immune activation in a tissue.
T cells (Th2/Tfh) help B cells produce IgG4 and other antibodies; cytotoxic T cells release tissue‑injury and pro‑fibrotic signals.
Eosinophils (when present) add allergic‑type inflammation.
Fibroblasts respond by laying down collagen, this leads to fibrosis.
Without treatment, the cycle can continue, leading to organ damage.
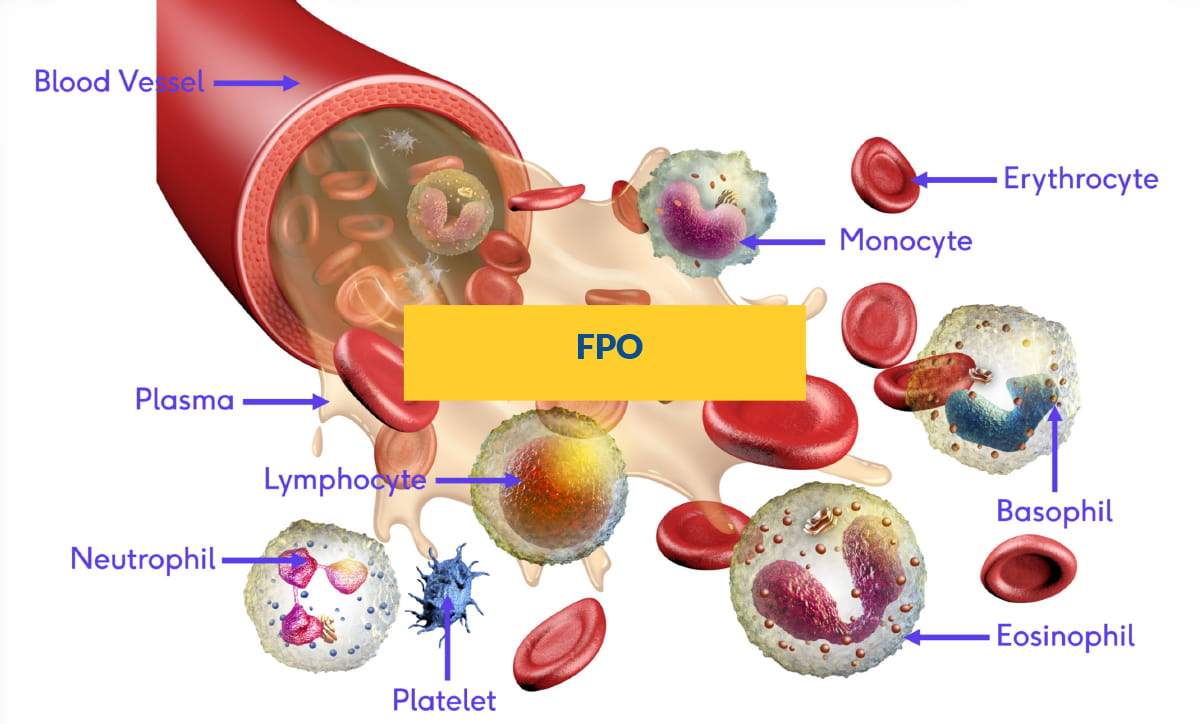
Other blood and plasma cells at a glance
B cells / plasma cells (subset of “lymphocytes”): Central to IgG4-RD—B cells mature into plasma cells that produce IgG4; pathology often shows IgG4-rich plasma cells in tissue.
Monocytes/macrophages: Cleanup crew and signalers; can secrete factors that nudge fibroblasts toward scar-building.
Neutrophils: First-responder infection fighters; not a hallmark of IgG4-RD tissue (usually scant)
Basophils: Allergy helpers that release histamine; a minor player compared with eosinophils.
Platelets: Clotting fragments; not central to IgG4-RD mechanisms.
Erythrocytes (RBCs): Oxygen carriers in blood.
Plasma: The liquid that carries proteins—including immunoglobulins—and is relevant when we talk about serum IgG4 blood tests
What your care team might check
Clinicians don’t rely on any single clue. They put together blood work, imaging, and—when safe—biopsy to see the full picture of cells and scarring.
Blood tests: Eosinophil count, IgE, and serum IgG4 (remember: IgG4 can be normal in confirmed IgG4‑RD). Clinicians may also monitor inflammation markers.
Imaging: Can show swelling, thickening, or narrowing near ducts and vessels.
Biopsy: When safe and possible, tissue is key. Pathology looks for IgG4‑rich plasma cells, storiform fibrosis, and obliterative phlebitis (veins narrowed by inflammation). ³
How treatments target these pathways
Treatment is about quieting the conversation between these cells and giving tissues time to heal. Different medicines turn down different “speakers” in the immune orchestra.
Glucocorticoids (steroids) calm many arms of the immune response and often shrink masses quickly.
B‑cell–directed therapy (such as rituximab/other agents) reduces B cells and the Tfh‑B‑cell “conversation,” often helping both inflammation and fibrosis risk.³–⁴
Steroid‑sparing medicines and emerging T‑ or cytokine‑targeted therapies are being studied to keep disease quiet with fewer side effects.
In summary
When the immune system’s neighborhood watch (T cells, eosinophils, fibroblasts, and their antibody creating B-cell partners) over-signals across the bloodstream and within tissues, their cross-talk can lead to inflammation and scarring. Understanding how this works can guide smarter testing and treatment.
As we’ve seen, T cells set the tone, eosinophils add intensity, and fibroblasts build the scaffolding that becomes fibrosis. These same signals also activate B cells. That's one reason steroids can quiet flares quickly and why B-cell–targeted therapies often work best when used early to protect organs.
T cells (Th2/Tfh, Tregs, cytotoxic) orchestrate the immune response and can promote fibrosis.
Eosinophils may amplify inflammation, especially in allergy‑linked cases.
Fibroblasts build scar‑like tissue (fibrosis) when driven by immune signals; this is often reversible with treatment.
References
1. Stone JH, Zen Y, Deshpande V. IgG4-Related Disease. N Engl J Med. 2012;366:539–551. URL: https://www.nejm.org/doi/10.1056/NEJMra1104650
2. Peyronel F, Della-Torre E, et al. IgG4-Related Disease and Other Fibro-Inflammatory Conditions. Nat Rev Rheumatol. 2025. URL: https://www.nature.com/articles/s41584-025-01240-x
3. Akiyama M, Alshehri W, et al. The Immunological Pathogenesis of IgG4-Related Disease Categorized by Clinical Characteristics. Immunological Medicine. 2025. URL: https://www.tandfonline.com/doi/full/10.1080/25785826.2024.2407224
4. Arias-Intriago M, Gomolin T, et al. IgG4-Related Disease: Current and Future Insights into Pathological Diagnosis. Int J Mol Sci. 2025;26:5325. URL: https://www.mdpi.com/1422-0067/26/11/5325