Bookmark this lesson
Login or create an account to save and access your bookmarks
Bookmark this lesson
Login or create an account to save and access your bookmarks
Not yet registered?
What you can access by simply creating a account:
Register today to get the most out of the education academy. Save your progress, bookmarks lessons, track your progress plus more...

Save your progress in this lesson so you can pick it up where you left off.

Add lessons to your bookmarks so you can quickly return to them in the future.

Track your progress throughout the course to see what you have achieved.
Understanding the disease
What IgG4-related disease is, why it can look like many other conditions, and how it affects the body.
 8 lessons
8 lessons Total: TBC
Total: TBC 10 minutes
10 minutesUnderstanding fibrosis
Understand fibrosis in IgG4‑RD, common warning signs, testing steps, and how early treatment can prevent damage.
When inflammation becomes scar: Understanding fibrosis in IgG4-related disease
When doctors talk about fibrosis, they mean extra scar‑like tissue that builds up in an organ. A little scar tissue can be helpful after injury. But too much can make an organ stiff and less able to do its job. In IgG4‑related disease (IgG4‑RD), the immune system causes long‑lasting inflammation that can lead to fibrosis in many parts of the body.
This lesson explains what fibrosis is, why it happens in IgG4‑RD, how doctors find it, and what treatments can help.
What is fibrosis?
Think of your body like a house that repairs itself. When there’s damage, your body sends in “patching material” to fix the spot. Fibrosis is when too much of that patching material builds up and makes the tissue stiff. A little is okay, but too much can cause trouble.
Fibrosis is the body laying down too much “patching material” (collagen) after inflammation or injury.
Extra scar tissue can narrow tubes (like bile ducts or ureters), thicken tissues (like around the eyes or lungs), and squeeze nearby structures.
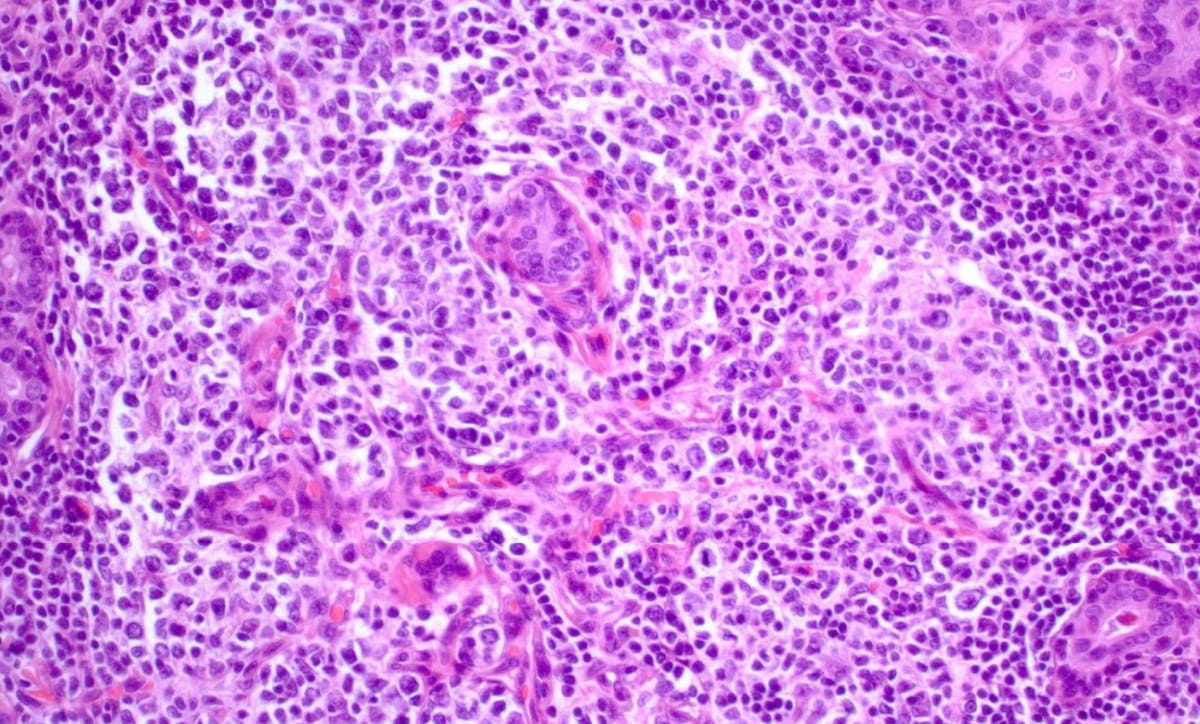
In IgG4‑RD, the fibrosis often has a special pattern called storiform fibrosis (it looks like swirling spokes under the microscope).1
How does IgG4‑RD lead to fibrosis?
When IgG4‑RD is active, the immune system stays “on” in certain organs. Immune cells gather in the tissue and release signals that tell repair cells to keep working. That steady signal means repair cells lay down more scar tissue than is needed. Over time, this can change how the organ looks and works.
Think of the immune system like a team that repairs a house. Some T cells act like over-eager foremen and cleanup crews: they send and respond to strong signals to "go build more patching material." In IgG4-RD, certain types (called cytotoxic CD4+ T cells and T follicular helper cells) can keep that repair switch stuck “on,” so extra scar builds up in specific organs more than others.2–3
When the immune system stays on too long, healing turns into scar.
On biopsy, doctors look for a classic trio: a dense mix of lymphocytes and plasma cells—many of them IgG4-positive—plus a storiform or “swirled-spoke” pattern of scar, and obliterative phlebitis, meaning small veins are partly or completely closed by scarring.1
Key features seen on biopsy:
Dense lymphoplasmacytic infiltrate rich in IgG4‑positive plasma cells.
Storiform fibrosis (swirled scar pattern).
Obliterative phlebitis (scarring around/inside small veins).
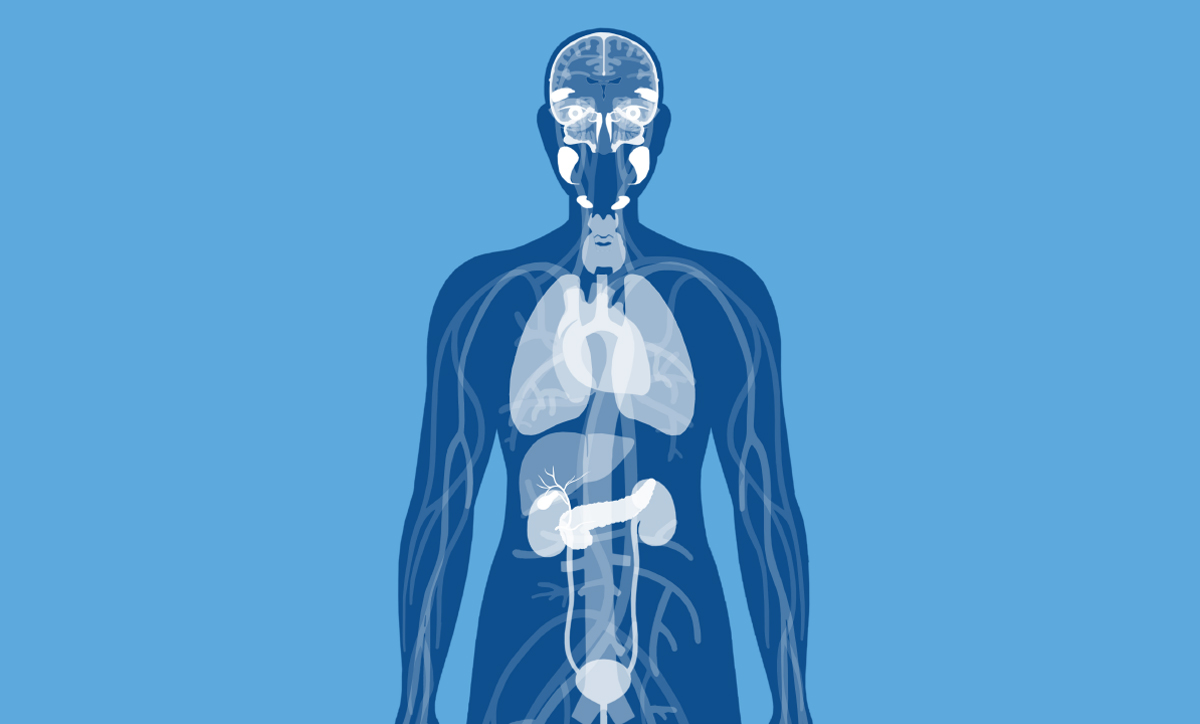
Where can fibrosis occur in IgG4‑RD?
IgG4-related disease is systemic, meaning it can affect many organs at once or over time. The most common areas include the pancreas and bile ducts; the retroperitoneum (the space behind the abdominal lining that contains the kidneys, ureters, adrenal glands, and the major blood vessels: aorta and inferior vena cava); and the salivary and lacrimal glands and tissues around the eyes.
What are signs and symptoms?
Because IgG4-RD can involve many organs, the symptoms can be different for every patient . A common clue is gradual swelling or blockage that develops over weeks to months rather than suddenly. Make a note of the onset, duration, and any change in daily function, and seek prompt evaluation if symptoms progress.
Some symptoms to watch for:
Jaundice (yellow eyes/skin), dark urine, pale stools when bile flow is blocked.
What this means: bile may be backing up from narrowed ducts. Be sure to note itching, right-upper-belly pain, and cholestatic labs; new jaundice warrants prompt evaluation.
Back/abdominal pain or reduced kidney function if ureters are compressed.
What this means: a fibrous “sheath” can pinch the tubes from kidney to bladder. Track urine output, blood pressure, and creatinine; consider imaging and stenting if obstruction is suspected.
Dryness, swelling, or bulging eyes with head-and-neck disease.
What this means: salivary/tear glands or tissues around the eye can enlarge. Watch for dry mouth/eyes, new double vision, or eyelid puffiness. Any vision change needs urgent ophthalmology review.
Shortness of breath or cough if the lungs are involved.
What this means: inflammation and scarring can stiffen lung tissue. Document onset, exercise tolerance, and fevers; consider chest imaging and pulmonary function testing if symptoms persist or progress.
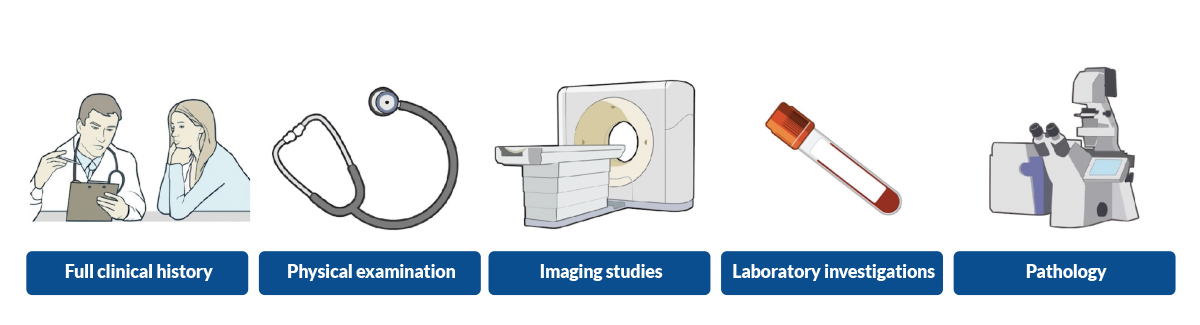
How do doctors detect fibrosis?
Doctors combine a patient’s history, physical examination, imaging of internal organs, and—when safe and appropriate—a small tissue sample (biopsy). Each element adds a piece to the puzzle, helping the care team confirm IgG4-RD patterns, gauge how much fibrosis is present, and choose the right treatment.
Blood tests: IgG4 level may be high, but this alone does not prove the diagnosis.
Imaging: CT/MRI/ultrasound can show thickening or masses and any squeezing of nearby tubes or vessels.
Biopsy (gold standard): Confirms the IgG4‑RD pattern and the amount of fibrosis.
Functional tests: For example, kidney blood tests or bile duct studies to see how well the organ works.
Can fibrosis be reversed?
Inflammation is easier to turn around than scar tissue. That’s why starting treatment early matters. Even when some scar remains, stopping further damage can protect how the organ works.
Established fibrosis may soften or shrink with treatment, but sometimes it remains. The main goals are to stop progression, relieve blockage, and protect organ function.1,5
Inflammation is more reversible than scar. Treating early inflammation can prevent or limit new scarring.
Treatment basics for fibro‑inflammatory disease in IgG4‑RD
Treatment usually starts by calming the immune system and, if needed, opening any blocked tubes. Your plan is tailored to your organs, your other health conditions, and how you respond.
Glucocorticoids (steroids): Often the first step. They reduce inflammation and can improve swelling and some scarring‑related narrowing.
B‑cell–targeted therapy (e.g., rituximab): Used when steroids are risky, not tolerated, or when disease comes back.1,5
Other steroid‑sparing medicines: Sometimes used to maintain remission.
Procedures for blockages:
Biliary or ureteral stents to relieve obstruction caused by fibrosis.
Surgery is uncommon but may be needed if scarring severely distorts anatomy or if cancer cannot be ruled out.
Close follow‑up: Regular visits and imaging help catch flare‑ups early and protect organs.
Living well with IgG4‑RD and fibrosis
In spite of IgG4-RD being a rare condition, it’s important to remember you are not alone. Many people live full lives with IgG4-RD by learning their warning signs and staying in close touch with their care team.
Be sure to report new symptoms quickly—such as jaundice, new or worsening pain, swelling, trouble urinating, or changes in vision—so problems can be treated before scarring causes lasting harm.
Follow your medication plan exactly and speak up about side effects. There are often safe adjustments that can help. Care is a team effort: rheumatology usually leads, with organ specialists involved as needed—gastroenterology for bile ducts and pancreas, nephrology for kidneys, ophthalmology for eye and orbit issues, and surgery or interventional procedures when blockages require relief. Regular check-ins, labs, and imaging help protect organ function over time.
The bottom line
Fibrosis is extra scar tissue that can build up after long‑lasting inflammation. In IgG4‑RD, unique immune patterns lead to scarring in different organs.
Early diagnosis, anti‑inflammatory treatment, and relief of any blockages help protect organ function. Some established scar may remain, but treatment aims to stop it from getting worse.
Inflammation is more reversible than scar. Treating early inflammation can prevent or limit new scarring.
References
1. Stone JH, Zen Y, Deshpande V. IgG4‑Related Disease. N Engl J Med. 2012;366:539–551. URL: https://www.nejm.org/doi/full/10.1056/NEJMra1104650
2. Peyronel F, Della‑Torre E, Maritati F, et al.IgG4‑related disease and other fibro‑inflammatory conditions. Nat Rev Rheumatol. 2025;21:275–290. URL: https://doi.org/10.1038/s41584-025-01240-x
3. Akiyama M, Alshehri W, Ishigaki S, et al. The Immunological Pathogenesis of IgG4‑RDCategorized by Clinical Characteristics.Immunological Medicine. 2025;48(1):11–23. URL: https://doi.org/10.1080/25785826.2024.2407224
4. Razok A, Romero Noboa ME, Sami F, et al. IgG4‑related disease and isolated retroperitoneal fibrosis: a narrative review. ARP Rheumatology. 2023;2:155–159. URL: https://www.arprheumatology.com/article/igg4-related-disease-and-isolated-retroperitoneal-fibrosis-a-narrative-review/
5. Lang D, Zwerina J, Pieringer H. IgG4‑related disease: current challenges and future prospects. Therapeutics and Clinical Risk Management. 2016;12:189–199. URL: https://doi.org/10.2147/TCRM.S99985